Treatment Non-Compliance Due to Glyceryl Trinitrate Side Effects in Anal Fissure
Bilal Ahmed,Khalid Farooq Danish ,Rehan Ahmed Khan,Muhammad Asad,Muhammad Ismail Seerat.
1Islamic International Medical College Trust, Pakistan Railway Hospital Rawalpindi¸ Rawalpindi
Objective: Anal fissures generally respond very well to the glyceryl trinitrate (GTN) ointment. However, it is associated with side effects like headache and hypotension.
Objective was to evaluate the noncompliance of patients to topical glyceryl trinitrate due to its side effect in the management of anal fissure.
Methodology:After taking ethical approval, a prospective case series was conducted at IIMCT-Pakistan Railway Hospital over a period from 1st March, 2023 to 31st August 2023. A sample size of 112 was calculated using WHO calculator 1.1 and these many patients were subsequently studied for side-effects of GTN and their compliance to the therapeutic regime.
Results:Of 122 patients studied: 62 (55.4%) were males, mean age was 35.35±10.22 years and mean daily doses of GTN was 2.31±0.56. Sixty-five (53%) of the patients using topical GTN reported side effects. Headache and postural hypotension were the most commonly reported side effects: 29.5% and 21.4% reported these side effects, respectively. Non-compliance was noted in only 14 patients (12.5%). Headache contributed 78.6% whereas postural hypotension & palpations contributed 21.4% towards the non-compliant cases. Thus, these two side effects were the only ones contributing towards non-compliance and had statistically highly significant association with non-compliance at a p value of 0.001. 94% of the compliant patient completely healed completely whereas only 2% of non-compliant patients achieved healing till 3-month follow-up: these results were significant at p<0.001.
Conclusion:Headache postural hypotension are significant side-effects of GTN; and they lead to non-compliance and thus subsequent failure to achieve healing.
Key words:Anal fissure, glyceryl trinitrate, headache, postural hypotension
Anal fissure, a term encompassing small cuts or tears in the anoderm, is a common condition. There are no reliable estimates of its incidence. Anal fissures are associated with reduced quality of life and intolerable pain.1It’s pathophysiology is associated with increased pressure at the ano-dermal muco-cutaneous lining. This increased local pressure has been held responsible for ischemia of the ano-dermal lining and thus inability of these ano-dermal tissues to proliferate at their normal rate.
The ischemia causes cellular necrosis that results in anal fissures and these don’t heal because of the same ischemic state of the ano-dermal lining,2 Since the anal fissures are painful, especially during defecation; patients try to delay bowel movements. This further worsen the condition by making stools harder and defecation more painful and traumatic to the ano-dermal lining. Multiple medical as well as surgical options have been utilized for the management of anal fissures. Among conservative management options, use of glyceryl trinitrate (GTN) ointment has been proved as an effective therapy.Glyceryl trinitrate ointment is a well-known nitric oxide donor that promotes anal fissure healing by decreasing resting anal pressure and increasing ano-dermal blood flow via the stimulation of intracellular cyclic guanosine monophosphate; resulting in reduction of cytosolic calcium.3,4 However this treatment is associated with various side effects due to which patients don’t comply. Headaches and postural hypotension are reported to be the most significant side effects.5 In a study by Emile et al, 30% of study population with anal fissures on GTN treatment had headaches and 25% had postural hypotension. Their results showed that 5 out of 65 patients (8%) withdrew GTN treatment for anal fissure due to the aforementioned side effects.6 The aim of this study was to evaluate the noncompliance of patients to topical glyceryl trinitrate due to its side effect in the management of anal fissure. There is very limited data available nationally as well as internationally to look for noncompliance of patients on GTN treatment due to its side effects. Our study aims to fill this literature gap. This study will help the surgeons to get better insight about GTN noncompliance in anal fissure and thus will help them tailor their practices.
After taking ethical approval from Institutional Review Committee of Islamic International Medical College, Riphah International University, Rawalpindi; a prospective case series was carried out at the surgical unit of IIMCT-Pakistan Railway Hospital.
The study period spanned over a 6 months period: starting from 1st March, 2023 to 31st August 2023. During the aforementioned period, consecutive sampling was done and all the patients attending out-patient or emergency department and getting diagnosed with anal fissure and subsequently put on GTN ointment were studied. A sample size of 112 was calculated using WHO calculator 1.1 and taking confidence level percentage (Z) as 1.96, anticipated population proportion as 8%6 and absolute precision required as 0.05%. Patients of all age groups and both genders were included. Whereas, all those patients taking analgesics to cover the side effects of GTN or as a prescription for any other condition like migraine, rheumatoid arthritis etc. were excluded from the study group. All the studied patients were briefed about the research methodology and after their consent, data was recorded by the primary researcher on pre-designed performas. The performa included spaces to record information regarding basic profile (name, age, sex, MR number), diagnosis, GTN use, GTN dosage, side effects experienced e.g., headache, nausea, vomiting, and compliance failure due to the side effects. SPSS 23 was used for data entry and analysis. Distribution of categorical and quantitative variables was analysed in terms of frequencies and measures of central tendencies respectively. Inferential analysis was performed by application of independent sample t test for quantitative variables and chi-square/Fischer’s exact test for categorical variables.
A total of 122 patients were studied: majority of the cases 62 (55.4%) were males. The mean age was 35.35±10.22 years and mean daily doses of GTN was 2.31±0.56. Detailed history revealed that more than half i-e 52.7% of the patients had chronic anal fissure and on examination vast majority i-e 81.3% had fissure posterior to the anal opening. Sixty-five (53%) of the patients using topical GTN reported side effects of the treatment. Here headache and postural hypotension were the most commonly reported side effects: 29.5% and 21.4% reported these side effects, respectively.
|
Table 1: Description of categorical variables |
||
|
Variable |
Categories |
Frequency (percentage) |
|
Gender |
Male |
62 (55.4) |
|
Female |
50 (44.6) |
|
|
Fissure’s chronicity |
Acute |
53 (47.3) |
|
Chronic |
59 (52.7) |
|
|
Fissure’s location |
Anterior |
21 (18.8) |
|
Posterior |
91 (81.3) |
|
|
Side effects |
Headache |
33 (29.5) |
|
Nausea |
2 (1.8) |
|
|
Vomiting |
3 (2.7) |
|
|
Peri-anal burning |
3 (2.7) |
|
|
Postural hypotension & palpitations |
24 (21.4) |
|
|
None |
47 (42) |
|
|
Non-compliant |
Yes |
14 (12.5) |
|
No |
98 (87.5) |
|
|
Fissure’s healed |
Yes |
95 (84.8) |
|
No |
17 (15.2) |
|
Non-compliance was noted in only 14 patients (12.5%). At 3-month follow-up, healing of the fissure was seen in 84.5% (95 cases). These results are summarized in tables 1. Whereas figure 1 summarizes the compliance status of the patients. It illustrates that 87% complied with the given GTN regime whereas 13% didn’t: 10% because of complaint of headache and 3% because of postural hypotension and associated palpitations. The studied patient and disease related variables were analysed to assess their relationship with the treatment non-compliance.
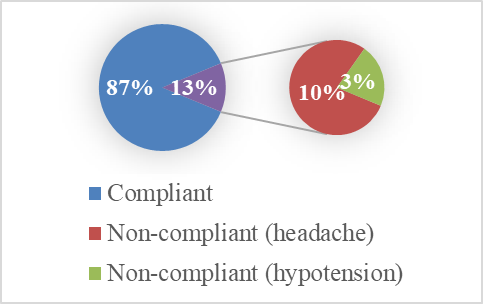
Table 2 summarizes that neither age nor daily doses of topical GTN were significantly associated with the treatment compliance. However, chi-square results summarized in table 3 depicted that 94% of the compliant patient had a completely healed fissure whereas only 2% of non-compliant patients achieved healing till 3-month follow-up. These results were highly significant with a p-value of <0.001. The only other variable that had significant association with GTN compliance was side-effects. Here, headache contributed 78.6% whereas postural hypotension & palpations contributed 21.4% towards the non-compliant cases. Thus, these two side effects were the only ones contributing towards non-compliance and had statistically highly significant association with non-compliance at a p value of 0.001. (Table 3)
|
Table 2: Independent sample t-test analysis of the data with respect to the compliance to GTN regime |
||||
|
Variable |
Complied with GTN regime |
Mean ± SD |
t- value (df) |
p-value |
|
Age (yrs.) |
Yes |
32±9.35 |
-1.318 (110) |
0.19 |
|
No |
35.83±10.29 |
|||
|
GTN doses |
Yes |
2.63±0.49 |
2.366 (110) |
0.20 |
|
No |
2.26±0.56 |
|||
One of the most common conditions that present with adulthood anal pain and bleeding is anal fissure. As per the duration of complaints, it is divided into acute and chronic fissure: with six weeks as the cut-off period between the two. Here the pathogenesis is that passage of hard stools causes minor tear in anoderm that is termed as an acute anal fissure. In majority of the cases, it heals without long term consequences. However, if the anoderm fails to do so it gets converted into chronic anal fissure. Persistent internal sphincter (IAS) spasm has been associated with this progression to the chronic anal fissure.7
This association of anal sphincter spasm with anal fissure has been explained for both the acute and chronic fissures.8 Functional spasm of IAS has role in pathogenesis of acute fissures. Whereas, in chronic fissure a constant state of hypertonicity of IAS as well as fibrosis contribute towards pathogenesis of the condition.9 This hypertonic state of IAS impedes blood supply of the already susceptible anoderm: thus, further aggravating the situation by delaying healing. Posterior anal commissure is the area where blood supply is already deficient: thus, the chronic anal fissure is more common posteriorly; and these are essentially ischemic ulcers that don’t heal on their own: as was proposed by Schouten and colleagues.2
The role of medical management is the mainstay in cases of acute anal fissures: 80% of these heal with the conservative treatment.8 The chronic fissures don’t respond that well to the conservative management. Literature has inferred that around only 8 to 52% chronic fissures heal with stool softeners and local anaesthetic agents. Between 40 to 69% of the chronic fissures heal with the topical GTN management: with a recurrence rate of up to 50%. Thus, irrespective of the type of the fissure medical management is the first choice for symptomatic relief in all the cases. This conservative management regime includes sitz baths, laxatives including high fibres diet and chemical sphincterotomy. Commonly used methods of chemical sphincterotomy include local agents as 0.2% GTN and 0.4% nifedipine (calcium channel blockers), as well as botulinum toxin.
GTN works by a very specific pathway. Nitric oxide has been observed by Lund to decrease the tone of IAS: this happens secondary to reduced activity of nitric oxide synthase. This phenomenon has led to the use of nitric oxide donors as GTN.3 Local applications of GTN works by two pathways: firstly, by relaxing the IAS and secondly by increasing the blood supply to the anoderm, both these effects are achieved by the release of nitric oxide.10 Thus, it promotes the healing of anal fissures. But this mechanism of action is also the pathway that leads to GTN’s side effects that include headache, postural hypotension and dizziness. Here, the objective was to look into the side effects that occurs with the topical use of GTN; and look into the role of these side effects in non-compliance with the GTN therapy. Here an important finding previously published is that GTN is less affective in chronic anal fissures and this results from poor absorption of GTN from the fibrosed anoderm: owing to the inability of fibrous tissue to absorb the compound.
Previously published literature has reported that the complications of topical GTN varies from 5.9% to 56.4%2 and as many as up to 60% of the patients suffer from headache.11-13 Our study revealed a figure of 53% as complication rate following topical GTN: this includes 33% incidence of headache and 24% incidence of postural hypotension and palpitations. The rest of the side effects in our study group included nausea, vomiting and peri-anal burning: all these made up a total of 8% of complications. These results are similar to the results published previously, that reported 30 % headache and 25 % postural hypotension. To avoid this headache, where agents including nifedipine, bethanechol and diltiazem have been used as an alternative of GTN.14
Here it is noteworthy that none of the patients included in our study group complained of incontinence. This is a significant finding as the other treatment modalities have been consistently associated with soiling with faecal matter. Seven percent of the population suffers from temporary incontinence following botulin toxin dosage.15 and this complication is as common as up to 30% in those undergoing lateral sphincterotomy.16 The inferential statistics of our project shows that 95% of the fissures healed till the 3-month follow-up when put on GTN ointment: thus, avoiding more aggressive management of lateral sphincterotomy that commonly lead to incontinence. However, the recurrence of fissure over long-term wasn’t assessed: however, guidelines for management for such recurrent patients include giving a second regime of the same GTN. It is noteworthy that good patient counselling regarding the recurrence and second attempt at healing with GTN application is important.
Study Limitations:
This study was a unicentric one and has no data regarding long-term follow-up of the patients: thus, recurrence can’t be properly assessed. Hence there is need of studies with a longer duration of follow-up to assess that effectivity of the GTN management and its side-effects; and hence delineate their role in non-compliance.
GTN therapy is associated with significant side-effects even when used for local application. Headache postural hypotension is among the significant side-effects of GTN; and they have been found to lead to non-compliance. Thus, the patients that suffer from these side-effects are prone to not achieve the healing of fissure.
- Jin JZ, Hardy M-O, Unasa H, Mauiliu-Wallis M, Weston M, Connolly A, et al. A systematic review and meta-analysis of the efficacy of topical sphincterotomy treatments for anal fissure. International Journal of Colorectal Disease. 2022;37(1):1-15. https://doi.org/10.1007/s00384-021-04040-3
- W.R. Schouten, J.W. Briel, J.J. Auwerda, E.J. De Graaf. Ischemic nature of anal fissure, Br. J. Surg. 83 (1) (1996 Jan) 63-5. https://doi.org/10.1002/bjs.1800830120
- Gallo G, Trompetto M, Fulginiti S, La Torre M, Tierno S, Cantarella F, et al. Efficacy and safety of Propionibacterium extract gel versus glyceryl trinitrate ointment in the treatment of chronic anal fissure: a randomized controlled trial. Colorectal Dis. 2023 Aug;25(8):1698-707. https://doi.org/10.1111/codi.16576
- Emile SH, Elgendy H, Elfeki H, Magdy A, Abdelmawla AA, Abdelnaby M, et al. Does the duration of symptoms of anal fissure impact its response to conservative treatment? A prospective cohort study. International Journal of Surgery. 2017; 44:64-70. https://doi.org/10.1016/j.ijsu.2017.06.044
- Anal fissure, Medscape [Database on the internet], https://emedicine.medscape.com/article/196297-overview#a9. Accessed on 5 May 2016. M. Farid, A. El Nakeeb, M. Youssef, et al. Idiopathic hypertensive anal canal: a place of internal sphincterotomy, J. Gastrointest. Surg. 13 (9) (2009) 1607-13, https://dx.doi.org/10.1007/s11605-009-0931-6.
- Bacher H, Mischinger H-J, Werkgartner G, Cerwenka H, El- Shabrawi A, Pfeifer J et al. Local nitroglycerin for treatment of anal fissures: an alternative to lateral sphincterotomy? Dis Colon Rectum 1997; 40: 840-5. https://doi.org/10.1007/bf02055444
- Khubchandani IT, Reed JF. Sequelae of internal sphincterotomy for chronic fissure in ano. Br J Surg 1989; 76: 431-4. https://doi.org/10.1002/bjs.1800760504
![]()
An Official Publication of
Islamabad Medical & Dental College
Volume 12 Issue 4
Editorial
Address of Correspondence
Dr. Bilal Ahmed
Email:
bilalbashir4568@gmail.com.pk
Cite this article.Ahmad B, Danish FK, Khan RA, Asad M, Seerat IM, Nisar UM. Treatment Non-Compliance Due to Glyceryl Trinitrate Side Effects in Anal Fissure. J Islamabad Med Dental Coll. 2023; 12(4): 270-275 DOI: https://doi.org/10.35787/jimdc.v12i4.1051