A Comparison of Hysterosalpingographic Results in Individuals Experiencing Primary and Secondary Infertility: A Prospective Approach
Naushaba Malik1Hinna Hanif Mughal2Hassan Mumtaz3Shahbakht Aftab4Saima Bibi6Rida Noor7
1Consultant Radiologist, PESSI Hospital, Islamabad, Pakistan & Islamabad Diagnostic Centre, Islamabad, Pakistan
2Benazir Bhutto Hospital, Rawalpindi, Pakistan
3BPP University, London, UK
4,7Postgradute Resident, Pakistan Institute of Medical Science, Islamabad, Pakistan
5House Officer, Pakistan Institute of Medical Science, Islamabad, Pakistan
6Assistant Professor, Dept of Obs & Gynae, Holy Family Hospital, Rawalpindi
Objective: This study aims to compare the HSG results in a study population having primary and secondary infertility.
Methodology:We conducted a one-year prospective study at Islamabad Diagnostic Center in Islamabad, Pakistan after getting institutional review board approval. Sample size was calculated using online software “Raosoft” which estimated it to 242. All the patients who gave informed consent and having primary and secondary infertility were enrolled. Demographics of the patients including age, duration of infertility, and the presence of tubal and uterine abnormalities, were collected by reviewing clinical notes and X-ray findings.
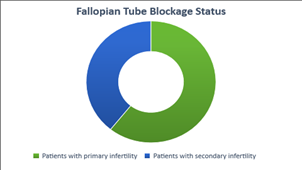
Results:Among 242 enrolled patients with infertility, the ratio of primary infertility was 70.27% (n=170) and that of secondary infertility was 29.75% (n=72). In both the groups, fallopian tube blockage was observed as a major abnormality that affected 20.00% (n=34/170) of patients with primary infertility and 30.55% (n=22/72) of patients with secondary infertility. Unilateral tube blockage was observed in 26.47% (n=9/34) whereas, bilateral blockage was observed in 29.41% (n=10/34) patients with primary infertility. 23.52% (n=8/34) of patients got affected with Bilateral hydrosalpinx, whereas unilateral loculated spill was perceived in 8.82% (n=3/34) patients
Conclusion: In this study, fallopian tube abnormalities were most predominant among barren women. So, taking deterrent actions and efficiently management of pelvic infections are indispensable in plummeting the manifestation of infertility resultant of the tubal issues.
Key words:Hysterosalpingography, Infertility, Subfertility, Tubal blockage.
The World Health Organization defines infertility as a disease of the reproductive system that makes it impossible to get pregnant after 12 months or more of regular unprotected sex. Infertility is a common problem affecting millions of people worldwide.1 Primary infertility is commonly believed to be more prevalent than secondary infertility, but a review of studies found that secondary infertility is actually more common, with a global incidence of around 15%.2
The rates of infertility have remained relatively steady over the past few eras, despite the global trend of preferring fewer children. People with a history of chlamydia infection, pelvic surgery, endometriosis, or Mullarian duct abnormalities may have a higher risk of subfertility.3,4
Tubal obstruction causes of infertility are more common in cases of secondary infertility, so routine fallopian tube evaluation is advisable for these cases.5,6 Polyps, irregularities in the uterine wall, fibroids, and congenital glitches contribute towards uterine causes of infertility. Up to 50% of patients facing repeated unsuccessful gestations have uterine abnormalities.4
Fallopian tube problems can cause infertility in up to 35-40% of people.7-9 They account for about 15-20% of primary infertility cases and up to 40% of secondary infertility cases. It's important for human fertility that the fallopian tubes stay open and work properly.10 These delicate tubes can be easily damaged by infections or surgery. This can affect the structure and function of the endosalpinx and fimbriae.
In Hysterosalpingography (HSG) test, a doctor assesses the size, structure and function of fallopian tubes, uterus and cervix. The test is comparatively safer and inexpensive in comparison with other available tests that are considered to estimate these reproductive organs. The sensitivity and specifity of HSG for detecting tubal blockages is around 65% and 83% respectively. Therefore, it is presumed that it can miss up to 35% of tubal blockages. HSG isn't as good at diagnosing problems outside of the fallopian tubes.11, 12
One can check the uterine and fallopian tube health using Hysterosalpingography (HSG) more reliably than any other test. It can also show if there are any abnormalities in the uterus, such as adhesions or birth defects. The inside morphology of the fallopian tube and the uterus can be best predicted with an examination with HSG. Moreover, the problems associated with the linings of the uterus can also be best assessed with the test. Though HSG is relatively inexpensive and safer test, some potential risks are also associated with it including exposure to radiation, infection, pain and discomfort.
This study aimed to compare the results of hysterosalpingography (HSG) tests in women suffering from primary and secondary infertility.
This prospective study was conceded at ‘Islamabad Diagnostic Centre’ Islamabad-Pakistan after getting approval from the institutional review board. The study was conducted from July 1, 2022 to June 30, 2023. The sample size was calculated using online software “Raosoft” which estimated it to 242. All the patients who gave informed consent and having primary and secondary infertility were enrolled. Demographic data, including age, duration of infertility, and the presence of tubal and uterine abnormalities, were collected by reviewing clinical notes and X-ray findings. Before the procedure, an informed consent was taken from all the study participants. The study included women between 20 and 45 years old who had both primary and secondary infertility for 1 to 15 years and had regular menstrual cycles. Similarly, women who had major surgery on their uterus and fallopian tubes were excluded from the study. Examinations with inconclusive results and studies that were not conducted for infertility were likewise eliminated from consideration.
The hysterosalpingography (HSG) procedure were performed 7-10 days after the patient's menstruation as at this time there is almost nil chance of conception. It is optional to have analgesic one hour prior to the procedure as advised by the gynecologist. Patients were positioned lying on their backs with their feet in stirrups (lithotomy position) on the X-ray table. A speculum inserted into the vagina to visualize the cervix. A 10F foleys catheter then carefully inserted into the cervix, ensuring a tight seal by inflating the bulb by distilled water (3-5 ml). 5-10ml water-soluble iodine containing contrast (urograffin) injected into the uterine cavity through the catheter. All procedure examined under fluoroscopic control. Usually four- six images of X-ray taken, including uterus fallopian tubes, and the spillage of contrast into the peritoneal cavity. A last X-ray image taken after removal of catheter.
Contraindications for this procedure included recent intrauterine interventions, current vaginal discharge or bleeding, prior salpingectomy, and a severe allergy to contrast material.
After data cleaning process, all the data was analyzed using statistical software SPSS version 24. We presented descriptive stats as frequency, mean and percentage. To determine if there were any notable differences, a chi-square test was utilized. A P value of ≤0.05 was considered statistically significant.
The study included women between 18 and 45 years (in various age groups) old who had both primary (m=170) and secondary infertility (n=72) for 1 to 15 years. The mean age of the participants was 28±2.00 years with primary infertility and 32±4.22 with secondary infertility. The results are displayed in figure 1. Primary infertility was present in 21.17% of individuals aged 18 to 22 (n=36), 69.14% in the 23-35 age group (n=118), and 9.4% in the 36-45 age group (n=16).
|
Table I: Types of Infertility in various age groups among the study participants. |
||||
|
Age Group |
Patients with Primary infertility |
% |
Patients with Secondary infertility |
% |
|
18-22 |
36 |
21.17 |
12 |
16.66 |
|
23-35 |
118 |
69.41 |
50 |
69.44 |
|
36-45 |
16 |
9,41 |
10 |
13.88 |
|
Total |
170 |
100 |
72 |
100 |
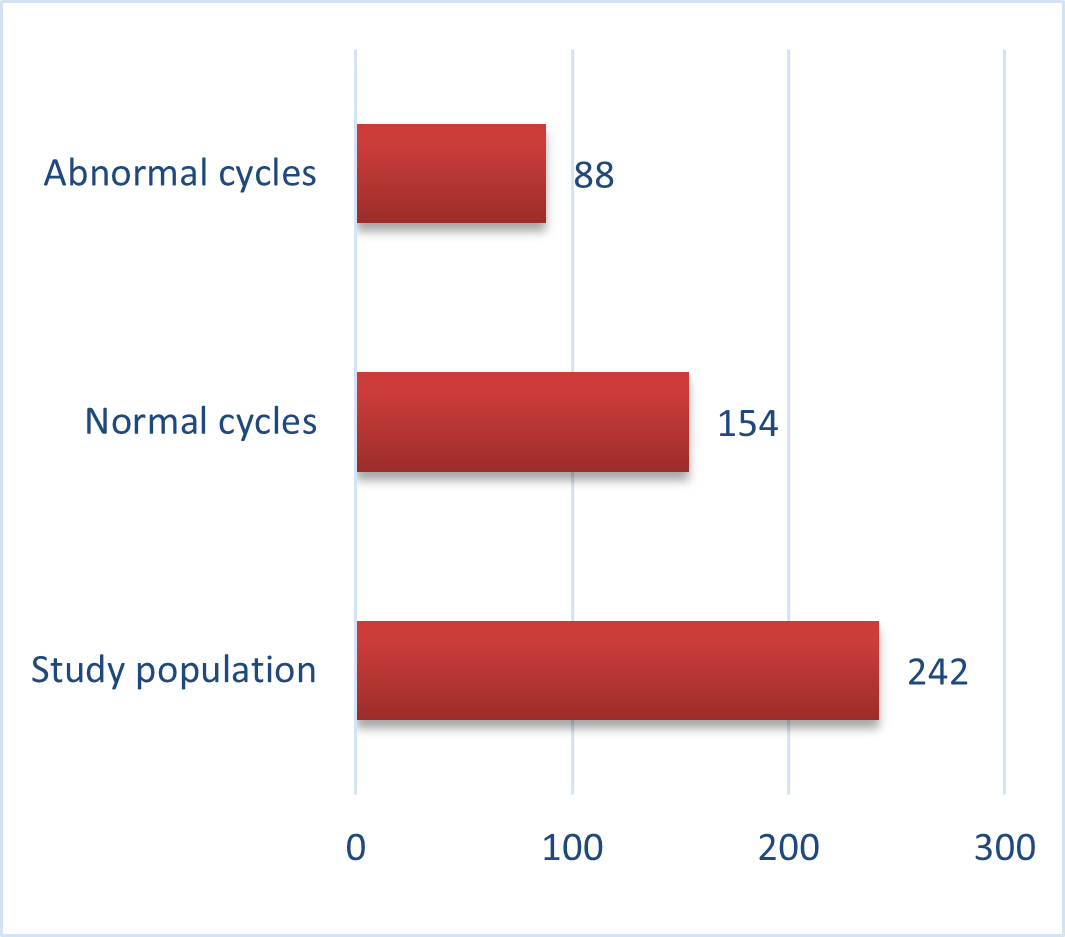
In the same manner, secondary infertility was observed in 16.66% of individuals aged 18-22 (n=12), 69.44% in the 23-35 age group (n=50), and 13.88% in the 36-45 age group (n=10). The results are shown in table 1. Out of 242 study participants, 63.63% (n=154) had regular periods, while 36.36% (n=88) had abnormal periods. The results are shown in figure 2.
Of all patients with primary infertility, 26.47% (n=9/34) had one-sided tubal blockage and 29.41% (n=10/34) had bilateral tubal blockage. Bilateral hydrosalpinx was found in 23.52% (n=8/34) of patients, and unilateral loculated spill was seen in 8.82% (n=3/34) of patients with primary infertility. In patients with uterine congenital abnormalities, 5.88% (n=2/34) had a bicornuate uterus, 2.94% (n=1/34) had a unicornuate uterus, and 2.94%



Figure IV: Photographs showing various complications
|
Table II: Hysterosalpingography findings of the study participants. |
|||
|
Complications |
Primary infertility |
Secondary infertility |
|
|
Fallopian tube blockage |
20.00% (n=34/170) |
30.55% (n=22/72) |
|
|
Unilateral tubal blockage |
26.47% (n=9/34) |
27.27% (n=6/22) |
|
|
Unilateral loculated spill |
8.82% (n=3/34) |
18.18% (n=4/22) |
|
|
Bilateral tubal blockage |
29.41% (n=10/34) |
18.18% (n=4/22) |
|
|
Bilateral hydrosalpinx |
23.52% (n=8/34) |
13.63% (n=3/22) |
|
|
Uterine Pathologies |
Unicornuate uterus |
2.94% (n=1/34) |
13.63% (n=3/22) |
|
Bicornuate uterus |
5.88% (n=2/34) |
4.54% (n=1/22) |
|
|
Uterine didelphys |
2.94% (n=1/34) |
4.54% (n=1/22) |
|
|
Normal |
136 (80.0%) |
50 (69.44%) |
|
|
Total |
170 (100%) |
72 (100%) |
|
Infertility is a major healthcare concern in Pakistan, as well as in developing countries around the world. It is the most common reproductive challenge, and the ability to have children is an important part of life, health, and marriage. A number of factors contributes towards the higher rates of infertility including poverty, lack of education, pollution, gender inequality, and infectious diseases. This has also worsened by the population control measures. In our society, having children is meticulously connected to happiness, social stability and overall health. So, being labelled as barren every so often leads to mental and social adverse outcomes. Causes of Infertility differ depending on the local population and geographical distribution. Consequently, it is significant to study local infertility factors and address them accordingly. Hysterosalpingography (HSG) has been used for over a century and is still the main imaging tool used to diagnose infertility.13 It is still a popular choice despite other, more complex methods being available because it is affordable, easy to access, minimally invasive, and easy to interpret.
Our study found that infertility is most common in women aged 23-35, which is the peak of their reproductive years. The prevalence of infertility varies around the world, but in our study, primary and secondary infertility were equally common. This differs from previous studies in Nigeria, Pakistan, and Saudi Arabia, where secondary infertility was more common, and from a study in India, where primary infertility was more common. We also found that the type of infertility is related to the patient's age. 13-15 our study showed the existence of both the types in an age group of 23-35 years.
Primary infertility patients are referred for hysterosalpingography earlier than secondary subfertility patients, possibly because they marry earlier and seek medical help sooner for social reasons.17-20
Of those who undergo hysterosalpingography, 80% of primary infertility patients and 69.44% of secondary infertility patients have normal results. This is consistent with previous studies, which have found that structural abnormalities of the uterus and fallopian tubes are more common in secondary subfertility patients.
Unilateral and bilateral tubal obstructions are predominant in women suffering from secondary infertility, as are uterine abnormalities. These increased rates of tubal and uterine abnormalities in secondary infertility patients may be due to factors such as PID (pelvic inflammatory disease) or previous surgical considerations.21
In disparity, unilateral and bilateral hydrosalpinx are more commonly seen in primary infertility patients. This might be due to a developed incidence of PIDs among younger patients with primary infertility.
In order to examine the uterine and fallopian tubes in women suffering from infertility, Hysterosalpingography (HSG) technique is commonly used. The technique is used to assess any blockages in the tubes or normal morphology of the uterus. In this study most common factor found in infertile women was fallopian tube abnormalities. So, taking deterrent actions and efficiently management of pelvic infections are indispensable in plummeting the manifestation of infertility resultant of the tubal issues.
- Sun H, Gong TT, Jiang YT, Zhang S, Zhao YH, Wu QJ. Global, regional, and national prevalence and disability-adjusted life-years for infertility in 195 countries and territories, 1990–2017: results from a global burden of disease study, 2017. Aging (Albany NY). 2019 Dec 12;11(23):10952.2. https://doi.org/10.18632/aging.102497
- Starrs AM, Ezeh AC, Barker G, Basu A, Bertrand JT, Blum R, Coll-Seck AM, Grover A, Laski L, Roa M, Sathar ZA. Accelerate progress—sexual and reproductive health and rights for all: report of the Guttmacher–Lancet Commission. The lancet. 2018 Jun 30;391(10140):2642-92. https://doi.org/10.1016/s0140-6736(18)30293-9 Deshpande PS, Gupta AS. Causes and prevalence of factors causing infertility in a public health facility. Journal of human reproductive sciences. 2019 Oct;12(4):287. https://doi.org/10.4103/jhrs.jhrs_140_18 Tamrakar SR, Bastakoti R. Determinants of infertility in couples. journal of Nepal Health research Council. 2019 Aug 7;17(1):85-9. https://doi.org/10.33314/jnhrc.1827
- Jabeen F, Khadija S, Daud S. Prevalence of primary and secondary infertility. Saudi J Med. 2022;7(1):22-8. https://doi.org/10.36348/sjm.2022.v07i01.004 Bhagavath B, Greiner E, Griffiths KM, Winter T, Alur-Gupta S, Richardson C, Lindheim SR. Uterine malformations: an update of diagnosis, management, and outcomes. Obstetrical & gynecological survey. 2017 Jun 1;72(6):377-92. https://doi.org/10.1097/ogx.0000000000000444
- Roomaney R, Kagee A. Salient aspects of quality of life among women diagnosed with endometriosis: A qualitative study. Journal of health psychology. 2018 Jun;23(7):905-16. https://doi.org/10.1177/1359105316643069
- Tamrakar SR, Bastakoti R. Determinants of infertility in couples. journal of Nepal Health research Council. 2019 Aug 7;17(1):85-9. https://doi.org/10.33314/jnhrc.1827 Onwuchekwa CR, Oriji VK. Hysterosalpingographic (HSG) pattern of infertility in women of reproductive age. Journal of human reproductive sciences. 2017 Jul;10(3):178. https://doi.org/10.4103/jhrs.jhrs_121_16
- Exalto N, Emanuel MH. Clinical aspects of HyFoSy as tubal patency test in subfertility workup. BioMed Research International. 2019 Jul 8;2019. https://doi.org/10.1155/2019/4827376 Sarac M, Koc I. Prevalence and risk factors of infertility in Turkey: evidence from demographic and health surveys, 1993–2013. Journal of biosocial science. 2018 Jul;50(4):472-90. https://doi.org/10.1017/s0021932017000244
- Campisciano G, Florian F, D'eustacchio A, Stanković D, Ricci G, De Seta F, Comar M. Subclinical alteration of the cervical–vaginal microbiome in women with idiopathic infertility. Journal of cellular physiology. 2017 Jul;232(7):1681-8. https://doi.org/10.1002/jcp.25806
- Adedigba J, Idowu B, Hermans S, Ibitoye B, Fawole O. The relationship between hysterosalpingography findings and female infertility in a Nigerian population. Polish journal of radiology. 2020 Apr 13;85(1):188-95. https://doi.org/10.5114/pjr.2020.94488
![]()
An Official Publication of
Islamabad Medical & Dental College
Volume 12 Issue 4
Editorial
Address of Correspondence
Naushaba Malik
Email:
doctor.Noshi100@gmail.com
Cite this article.Malik N, Mughal HH, Mumtaz H, Aftab S, Khan MA, Bibi S, Noor R. A Comparison of Hysterosalpingographic Results in Individuals Experiencing Primary and Secondary Infertility: A Prospective Approach. J Islamabad Med Dental Coll. 2023; 12(4):310-316. DOI: https://doi.org/10.35787/jimdc.v12i4.1053