Effects of Decompression Therapy in Leg Pain and Straight Leg Raise in Patients with Lumbar Radiculopathy Due to Disc Protrusion
Abdul Ghafoor Sajjad1Muhammad Shahid Javed2Iqra Hamid3Syed Ali Hussain4Muhammad Ali Raja5Benish Shahzadi6
1Department of Allied Health Sciences, Sargodha Medical College, University of Sargodha
2Department of Physiology, Sargodha Medical College, University of Sargodha
3Max Physical Therapy and Rehabilitation Center, Max Health Hospital, Islamabad
4Department of Rehabilitation Sciences, Shifa Tameer e Millat University, Islamabad
5Small Heath Primary Care Network, Birmingham, UK
6Cromwell Health, Cromwell, Central Otago, New Zealand
Objective: The purpose of this study was to compare the effect of lumbar spine decompression therapy and standard physical therapy treatment in patients with lumbar radiculopathy due to disc protrusion.
Methodology:The single-blind randomized control trial of 71 patients was conducted at Max Rehab & Physical Therapy Centre Islamabad, Pakistan. After setting inclusion criteria all the patients were randomly allocated into treatment and control group. Both groups received standard physical therapy treatment including, Moist Hot Pack, Lumbar Mobilization, Stretching and strengthening exercises. The only difference was that Decompression Group received additional Decompression therapy.
Results:The data included demographics and Numeric Pain Rating Scale (NPRS) score in supine lying position for the painful leg and Straight Leg Raise (SLR) Range for the painful side. The values for leg pain for control group decreased from 6 to 3 and the value for straight leg raise increased from 15° to 49°. The values for leg pain for the Decompression Group decreased from 6 to 2 and the value for the straight leg raise increased from 10° to 48°, the p value for both the variables was <.001 showing statistically significant difference between pre and post values in treating patients leg pain and straight leg raise range of motion.
Conclusion: It is concluded that decompression therapy is more effective in managing lumbar radiculopathy.
Key words:Decompression, Disc Protrusion, Exercises, Low back pain, Lumbar radiculopathy
The most prevalent musculoskeletal issue in the modern world is low back pain.1 Nearly everyone has low back discomfort at some point in their lives, according to reports. In the fourth to eighth decades of life, it is most common. Women are more likely than men to experience low back discomfort.2 Low back discomfort may originate in the low back alone or may radiate to the lower extremities. Radiculopathy refers to pain that radiates down the extremities. Lumbar intervertebral disc pathology is a primary cause of lumbar radiculopathy, as it applies pressure to the spinal nerve that exits the body. Radiculopathy is the term for the pain that radiates along the nerve's route due to compression.3
The treatment of lumbar radiculopathy is divided in to two main types conservative and surgical. It is recommended that the initial management of lumbar radiculopathy has to be conservative and if the method fails then it patient is selected for surgical treatment.4 One of the most preferred and indicated conservative method of treating lumbar radiculopathy is spinal traction.5 This method of treatment is not new, it is reported that this form of treatment was used as in the form of “falling ladder” 3000 to 400 BC.6
It was Hippocrates who documented the spinal traction for the first time in his book called as “Peri Arthron”.7The process of suspension was in use till the first decades of the 20th Century after which it was replaced with spinal traction.8 The process of traction involves pulling the spine to cause negative pressure on the intervertebral disc that centralizes the nuclear material of the disk. The traction has been in the process of evolution since time and one of the most recent advancements in the spinal traction is the incorporation of motorized traction which is also called as non-surgical spinal decompression therapy (NSD).9 It has been used as a medical intervention to correct spinal deformities since early antiquity, it was in only 1950s and 1960s that lumbar traction became a popular treatment method for lumbar disc herniation (LDH) with contribution of James Cyriax.10In the non-surgical spinal decompression therapy, the computer has been added, which gauges and senses the traction force using specialized sensors and then adjusts the force required. It has provided a more sophisticated control of the forces exerted.11 The System Decompression Reduction Stabilization (DRS) is a machine which can exert traction forces and provide distraction at any targeted segment, thus providing more localized control of forces. This is achieved by creating a combination of specific angulation at the lumbar spine and varying amount of force that causes traction and thus decompressing the spine.12 It in year 1985 the American Doctor Allan Dyer first developed the spinal decompression machine, Furthermore the next six years he also worked the first computerized spinal decompression table. He named it the Vertebral Axial Decompression Therapy Table which is also known as Vax-D.13 There are different models of spinal decompression therapy systems are available like DRX-9000 and Spine Med Express. These units are quite expensive and they are most commonly used to treat cervical and low back pain of discogenic origin.
The decompression therapy tables usually have harnesses to strap up the patient and adjustable bolsters or pommels to hold the patient’s cervical spine or pelvis. These sites are used to create the pull. Unlike traditional spinal traction the spinal decompression therapy is progressive in nature, it is divided into cycles that are progressive (i-e increased pulling) and regressive in nature. The total duration of treatment may range from 10 minutes to half an hour. The force of traction increases gradually and the patient can stop the unit at any time using the hand-held emergency stop button.14 If we compare the cost of treatment, we can clearly see that the spinal decompression therapy is very economical as compared to the spinal surgery for degenerative disc disease or disc herniation or prolapse. These two conditions are most prevalent cause of spinal pain as well. The spinal decompression therapy causes a reduction in the intra-discal pressure.15 In this study the authors compared traditional physical therapy treatment for lumbar radiculopathy with spinal decompression therapy on the basis of Numeric Pain Rating Scale for Leg Pain and Straight Leg raise range of motion.
It was a registered randomized controlled trial having ethical letter number RIPHAH/RCRS/REC/Letter-00406 and was registered on US Clinical Trail registry. The RCT no was NCT04760210. Sample size for study was calculated through ‘Open-Epi’ tool with 95% confidence level (CI) and 5% precision error.16The patients were randomly assigned in two different groups through random lottery method.
The duration of this from April 2018 to September 2020. Study was conducted at Max Decompression & Physical Therapy Center, Max Health Hospital Sector G-8 Islamabad, Pakistan. The Max health hospital is private teaching hospital of Riphah International University Islamabad.
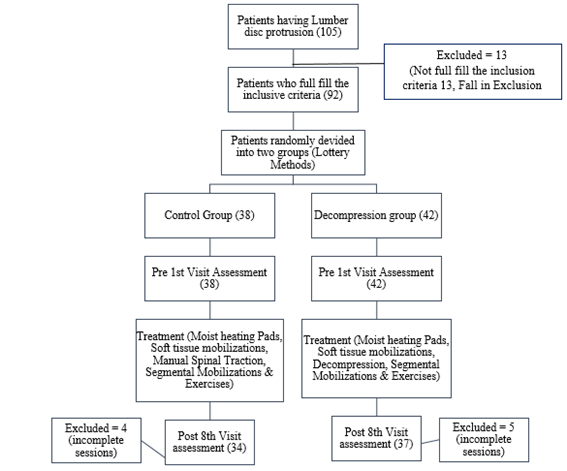
Initially 105 patients were recruited for the study, only 92 full fill the inclusion criteria which was; with minimum age limit of 30 years and maximum age limit is 60 years, both genders (Male and Female), Patients having complaint of localized and radiating pain of lumbar spine, Subjects having prolapsed intervertebral disc (PIVD) lumber disc bulging confirmed through Magnetic Resonance Imaging (MRI) were included in the study.
The exclusion criteria were those with a history of lumber disc surgery, lumbar spondylolisthesis, Lumbar spine fractures, Spinal stenosis, Spinal tumors, ankylosing spondylitis, and those using anticoagulants. Those participants who fall under the inclusion criteria were excluded from the study.
All the participants were volunteers and have given written permission to be a part of this study.Patients were divided in to two group’s control and decompression group through Randomization. The method of randomization was Lottery method. Patients were treated for 8 sessions; the sessions were given on alternate days. Both group received standard physical therapy treatment including Moist Hot pack for 10 minutes on lumber spine, Kaltenborn lumber paraspinal soft tissue mobilization, Maitland manual lumber spine traction, Maitland Lumbar Mobilization techniques including central posterior anterior mobilization, unilateral posterior anterior mobilization and rotation mobilization(each technique have 3 sets of 10 repetitions in each set), Calf, Hamstring and back extensors stretching exercises (3 sets of 10 repetitions), Strengthening exercises included bridging, SLR, prone hip extension, prone back extension (3 sets of 10 repetitions). The Stretching and strengthen exercises were also advised for home. The Decompression Group along with the standard physiotherapy session for 30 minutes treatment with additional decompression therapy. The data was collected on structured questionnaire. The data was collected 1st visit before intervention and after 8th visit of therapy. The data included demographics and Numeric Pain Rating Scale score, NPRS use to describe the pain intensity, the patient was asked about how they grade their pain from 1 to 10. The other variable is SLR, when there is radiculopathy, the patient was unable to raise its leg due to stretching pain of sciatica nerve. The SLR was measure on painful side radiculopathy. CONSORT diagram representing the whole procedure is given in Fig. 1.
According to shapiro wilk test value the data was not normally distributed, so we apply Mann-Whitney U test for inter group analysis and Wilcoxon Sign Rank Test for within group analysis in SPSS version 21.
The mean age of the participants was 44.78 ± 13.42 years. Among 71 participants the 41 were male and 30 were female. The 43.3% were house wife and 36.7% were office workers. Mostly participants had onset of pain more than one year (60%), 21.7% have pain less than 6 months and 18.3% have pain from less than 12 months. The percentage of radiculopathy due to PIVD in right leg was 72.5 and in left leg were 27.5. The highest dermatome level was L5-S1, which was 65.8%. the dermatome level confirms the involvement of lumbar spinal segment of disc protrusion (Table 1).
Table 1 Wilcoxon Sign Rank Test Inter Group Analysis
The data was not normally distributed so non-parametric statistical test Wilcoxon sign rank test was applied for inter group analysis. In non-parametric test we used median value instead of mean and inter quartile range in replacement of standard deviation.
In control group the straight leg rise range and pain in the leg was improve and show significant difference between pre 1st visit and post 8th visit treatment. The pre median (IQR) score of SLR was 15 (5) and Post Median (IQR) was 49(18), having the p-value < .001. The pre median (IQR) score of leg pain was 6(2) and Post Median (IQR) was 3(1), having the p-value < .001. In Decompression group the straight leg rise range and pain in the leg was improve and show significant difference between pre 1st visit and post 8th visit treatment. The pre median (IQR) score of SLR was 10(5) and Post Median (IQR) was 58(10), having the p-value < .001. The pre median (IQR) score of leg pain was 6(0) and Post Median (IQR) was 2(0), having the p-value < .001. (Table 2). The mann-whitney u test was applied between group analysis. At the base line before the treatment of 1st visit the p-value shows that there was no significant difference.
The Pre-SLR Median (IQR) value of control group was 15 (5) and Decompression group was 10(5) having p-value .121. The Pre NPRS (leg pain) Median (IQR) value of control group was 6(2) and Decompression group was 6(0) having p-value .137. After the 8th visit p-value shows that there was a significant difference. The Post SLR Median (IQR) value of control group was 49(18) and Decompression group was 58(10) having p-value less than .001. The Post NPRS (leg pain) Median (IQR) value of control group was 3(1) and Decompression group was 2(0) having p-value less than .001. (Table 3).
|
Table 1: Demographic Result of the Data |
|||||
|
S. No |
Variables |
Sub Variable |
Control (%) N=34 |
Decompression (%) N=37 |
Overall (%) N=71 |
|
1. |
Age |
Age (Years) |
42.28 ± 14.69 |
47.27 ± 11.61 |
44.78 ± 13.42 |
|
2. |
Gender |
Male |
20 |
21 |
41 |
|
Female |
14 |
16 |
30 |
||
|
3. |
Occupation |
House Wife |
50.0 |
36.7 |
43.3 |
|
Office Worker |
43.4 |
30 |
36.7 |
||
|
others |
5.6 |
33.4 |
20 |
||
|
4. |
Onset of Pain |
Less than 6 months |
30.0 |
13.3 |
21.7 |
|
Less than 12 months |
10.0 |
26.7 |
18.3 |
||
|
More than a year |
60.0 |
60.0 |
60 |
||
|
5. |
Unilateral involve leg |
Right Leg |
88.3 |
56.7 |
72.5 |
|
Left Leg |
11.7 |
43.3 |
27.5 |
||
|
6. |
Dermatome |
L3-L4 |
3.3 |
6.7 |
5 |
|
L4-L5 |
28.3 |
20.0 |
24.2 |
||
|
L5-S1 |
68.3 |
63.3 |
65.8 |
||
|
Table 2: Wilcoxon Sign Rank Test Inter Group Analysis |
||||||
|
S. No |
Variable |
Groups |
Pre Median (IQR) |
Post Median (IQR) |
Mean Rank |
P-Value |
|
1. |
SLR Range |
Control |
15 (5) |
49(18) |
30.5 |
<0.001 |
|
Decompression |
10(5) |
58(10) |
30.5 |
<0.001 |
||
|
2. |
NPRS (Leg Pain) |
Control |
6(2) |
3(1) |
30.5 |
<0.001 |
|
Decompression |
6(0 ) |
2( 0) |
30.5 |
<0.001 |
||
|
Table 3: Mann-Whitney U Test Between Group Analysis |
|||||
|
S. No |
Variable |
Groups |
Mean Rank |
Median (IQR) |
P-Value |
|
1. |
Pre SLR Range |
Control |
65.30 |
15 (5) |
.121 |
|
Decompression |
55.7 |
10(5) |
|||
|
2. |
Post SLR Range |
Control |
51.02 |
49(18) |
.003 |
|
Decompression |
69.68 |
58(10) |
|||
|
3. |
Pre NPRS (Leg Pain) |
Control |
64.83 |
6(2) |
.137 |
|
Decompression |
56.17 |
6(0 ) |
|||
|
4. |
Post NPRS (Leg Pain) |
Control |
76.71 |
3(1) |
.000 |
|
Decompression |
44.29 |
2(0) |
|||
The aim of current study was to determine how standard physical therapy treatment and with addition of spinal decompression therapy has an effect on leg pain and straight leg raise (SLR) range of patients with lumbar disc pathology. Findings of our study shows that values for leg pain and straight leg raise range of motion changed from baseline to the end of 8th session. The p value for both the variables was <0.001 showing statistically significant difference between pre and post values of both groups, however post values of intervention shows that decompression therapy was more effective in managing patients leg pain and straight leg raise range of motion.
It is clear from the cited sources that lumbar traction, decompression therapy, has been investigated in relation to lumbar disc protrusion. Research has examined the effectiveness of several traction methods and how they affect pain and functional improvement in individuals suffering from lumbar disc protrusion. The results of these investigations show good results of lumbar traction for the treatment of lumbar disc protrusion. showed that in patients with lumbar intervertebral disc degeneration, traction therapy produced more improvements in pain, function, and the morphology of the central canal area of the spine than did typical axial traction procedures.17 The lumbar disc protrusion may benefit from traction therapy, especially posterior-to-anterior traction. Traction decompression was recommended as a further physical therapy technique for lumbar disc herniation.18 In a meta-analysis. In relation to the management of lumbar disc protrusion, this meta-analysis offers additional evidence in favor of traction decompression as a possible therapeutic option for lumbar disc herniation. discovered that in individuals with acute low back pain, supine lumbar traction combined with traditional physical therapy decreased the size of herniated discs, decreased discomfort, and enhanced functional ability.19 This work sheds insight on the possible benefits of supine lumbar traction for managing lumbar disc protrusion, including pain reduction and improved functional ability outlined how spinal traction helps to manage lower back pain by progressively distracting spinal tissues into better alignment, lowering intervertebral disc pressure, and providing continuous or intermittent stretching axial force to the lumbar vertebrae.20
This focuses on how spinal traction works mechanically to reduce lower back pain, which is important for managing lumbar disc protrusion. In conclusion, the data from these studies provide credence to the idea that lumbar traction may help patients with lumbar disc protrusion have less discomfort and better functional outcomes. The results imply that traction therapy, namely supine lumbar traction and posterior-to-anterior traction, may be useful in regulating the morphology of the central canal area of the spine in people with lumbar disc protrusion, as well as in lowering pain and increasing function. The result of these studies supports our result that the decompression therapy improved the pain in lumber disc protrusion.
Choi et al., reported that in patients with intervertebral disc herniation general traction therapy and spinal decompression therapy are helpful in reducing pain and disability and improving Straight leg raise.21 Kang et. al reported that in patients with lumbar disc herniation, manual therapy and spinal decompression therapy are effective in improving Straight leg raise angle.22 Lee et al concluded that combined manual mobilization and spinal decompression therapy was more effective in reducing pain, improving range of motion as compared to standard physical therapy protocol with spinal decompression therapy.23 The values for leg pain for the Decompression Group decreased from 5.9 to 1.9 and the value for the straight leg raise increased from 12.42° to 56.15°, the p value for both the variables was <0.001 showing statistically significant difference between pre and post values showing that decompression therapy was effective in managing patients leg pain and straight leg raise range of motion. Finding of our study shows the values for leg pain for control group decreased from 6.07 to 2.38 and the value for straight leg raise increased from 13.13° to 50.08°. The values for leg pain for the Decompression Group decreased from 5.9 to 1.9 and the value for the straight leg raise increased from 12.42° to 56.15°, the p value for both the variables was <0.001.
In 2008 kim Hee Snag et al concluded that for lumbar disc pathologies and pain, one of most effective treatment option was spinal decompression therapy. He reported mean Visual analog scale values for spinal decompression therapy group was reduced from 6.9±1.86 to 2.6±1.43 and mean value of intermittent mechanical traction group was reduced from 6.4±1.28 to 4.5±1.22.24
According to Thomas F: Meszaros lower extremity mobility can be improved with traction during straight leg raise. Traction with body weight of 30% and 60% were effective for improving range of motion. In comparison to pretraction level the lumbar spine traction shows significant improvement in straight leg raise.25
Ma et al., concluded that combination of Spinal decompression therapy and therapeutic modalities shows significant improvement in straight leg raise after 10 and 20 treatment sessions. It is reported that therapeutic modalities in combination of Spinal decompression therapy is effective, safe, and non-invasive intervention in lumbar radiculopathy patients.26
It is concluded that additional decompression therapy was more effective in managing patient’s leg pain and straight leg raise range of motion as compared to standard therapy of patients with radicular pain due to lumbar disc protrusion.
- Sant’Anna PCF, Morimoto T, Miranda FdS, Garcez AdS. Low back pain in university students: what is the impact of COVID-19 pandemic?Fisioterapia e Pesquisa. 2022;29:284-90. https://doi.org/10.1590/1809-2950/22010929032022EN
- Bikbov MM, Kazakbaeva GM, Zainullin RM, Salavatova VF, Gilmanshin TR, Arslangareeva II, et al. Prevalence of and factors associated with low Back pain, thoracic spine pain and neck pain in Bashkortostan, Russia: the Ural Eye and Medical Study. BMC Musculoskeletal Disorders. 2020;21(1):1-14.
- Chandankhede AR, Talwar D, Acharya S, Kumar S. Spontaneous Recovery in Complete Foot Drop in a Case of Lumbar Disc Herniation: A Neurological Surprise. Cureus. 2022;14(1). https://doi.org/10.7759%2Fcureus.20962
- Stochkendahl MA-O, Kjaer P, Hartvigsen J, Kongsted A, Aaboe J, Andersen M, et al. National Clinical Guidelines for non-surgical treatment of patients with recent onset low back pain or lumbar radiculopathy. (1432-0932 (Electronic)). https://doi.org/10.1007/s00586-017-5099-2
- Vasiliadis ES, Grivas TB, Kaspiris A. Historical overview of spinal deformities in ancient Greece. Scoliosis. 2009;4:6-. https://doi.org/10.1186/1748-7161-4-6 Grimsby O. Clinical and Scientific Rationale for Modern Manual Therapy. San Diego: Ola Grimsby Institute San Diego; 1998.
- Daniel DM. Non-surgical spinal decompression therapy: does the scientific literature support efficacy claims made in the advertising media? Chiropractic & Osteopathy. 2007;15(1):1-5. https://doi.org/10.1186/1746-1340-15-7
- Yoon Y-S, Lee J-H, Lee M, Kim K-E, Jang H-Y, Lee K-J, et al., editors. Mechanical changes of the lumbar intervertebral space and lordotic angle caused by posterior-to-anterior traction using a spinal thermal massage device in healthy people. Healthcare; 2021: MDPI. https://doi.org/10.3390/healthcare9070900
- Wang W, Long F, Wu X, Li S, Lin J. Clinical efficacy of mechanical traction as physical therapy for lumbar disc herniation: a meta-analysis. Computational and Mathematical Methods in Medicine. 2022. https://doi.org/10.1155%2F2022%2F5670303
- Khan RR, Riaz S, Rashid S, Sulman M. Effectiveness of mechanical traction in supine versus prone lying position for lumbosacral radiculopathy. Pakistan Journal of Medical Sciences. 2021;37(5):1451. https://doi.org/10.12669%2Fpjms.37.5.4200
- Cardoso L, Khadka N, Dmochowski JP, Meneses E, Lee K, Kim S, et al. Computational modeling of posteroanterior lumbar traction by an automated massage bed: predicting intervertebral disc stresses and deformation. Frontiers in Rehabilitation Sciences. 2022;3:931274. https://doi.org/10.3389/fresc.2022.931274
- Lee Y, Lee C-R, Cho M. Effect of decompression therapy combined with joint mobilization on patients with lumbar herniated nucleus pulposus. Journal of physical therapy science. 2012;24(9):829-32. https://doi.org/10.1589/jpts.24.829 Kim HS, Yun DH, Huh KY. Effect of Spinal Decompression Therapy Compared with Intermittent Mechanical Traction in Lumbosacral Disc Herniation. Journal of the Korean Academy of Rehabilitation Medicine. 2008;32(3):319-23
- Ma S-Y, Kwon W-A, Lee J-H, Min D-G. The effects of spinal decompression combined with therapeutic modalities for patients with lumbar radiculopathy. Journal of the Korea Academia-Industrial cooperation Society. 2013;14(1):336-43. http://dx.doi.org/10.5762/KAIS.2013.14.1.336
![]()
An Official Publication of
Islamabad Medical & Dental College
Volume 12 Issue 4
Editorial
Address of Correspondence
Abdul Ghafoor Sajjad
Email:
abdulghafoorsajjad@yahoo.com
Cite this article.Sajjad GA, Javed SM, Hamid I, Hussain AS, Raja MA, Shahzadi B. Effects of Decompression therapy in leg pain and straight leg raise in patient with lumbar radiculopathy due to disc protrusion. J Islamabad Med Dental Coll. 2023; 12(4): 336-344. DOI: https://doi.org/10.35787/jimdc.v12i4.1058.