A Unique Case Report of Heterotopic Pregnancy
Saba Khilji1Wajeeha Anum2Mehwish Tabassum3Aleena Tahir4Manal Niazi5Naeemah6
1Department of Radiology, Dr. Akbar Nizai Teaching Hospital, Islamabad, Pakistan
Heterotopic pregnancy, characterized by simultaneous intrauterine and extra uterine pregnancies, is a rare but potentially life-threatening condition. Its incidence has increased, attributed to factors such as pelvic inflammatory disease, and assisted reproductive technologies. We present a case of spontaneous heterotopic pregnancy in a 28-year-old woman with lower abdominal pain. Initial examination revealed a ruptured left tubal ectopic pregnancy alongside a live intrauterine pregnancy. Prompt diagnosis via transvaginal ultrasonography led to emergency laparotomy, confirming sonographic findings. The ruptured ectopic pregnancy was successfully removed, preserving intrauterine gestation. Follow-up ultrasounds demonstrated a progressing intrauterine pregnancy. This case underscores the diagnostic challenges and emphasizes the importance of early recognition and intervention in heterotopic pregnancies, especially in the absence of predisposing risk factors. Increased awareness, thorough pelvic examination, and close follow-up are crucial for optimal outcomes in both pregnancies.
Key words:Heterotrophic pregnancy, ectopic pregnancy, transvaginal ultrasound, laparotomy.
A heterotopic pregnancy is an uncommon occurrence in which there are at least two simultaneous pregnancies developing at separate implantation sites, with one of them intrauterine.1 Medical specialists and obstetricians are less likely to include heterotopic pregnancy in their differential diagnosis when the patient’s acute complaints are abdominal pain and vaginal bleeding [2] as the frequency of this condition ranges from 1 in 30,000 during a natural cycle to approximately 1 in 100 in assisted reproductive procedures.1 HP has increased over the past few decades. Many factors, such as the increased prevalence of pelvic inflammatory disease (PID) and the prolonged use of assisted reproductive technologies (ARTs), have been linked to this increased frequency.3 Delays in diagnosis can raise the morbidity and mortality risk for mother and intrauterine pregnancy.5The diagnosis of heterotopic pregnancy is challenging and is primarily made by transvaginal ultrasonography. Its low sensitivity persists, yet the diagnosis is frequently neglected or missed.2 The primary course of treatment is to remove the ectopic pregnancy while preserving the intrauterine one.4
This case report is of spontaneous heterotopic pregnancy presenting with a live 6-week intrauterine pregnancy and a ruptured left tubal ectopic pregnancy.
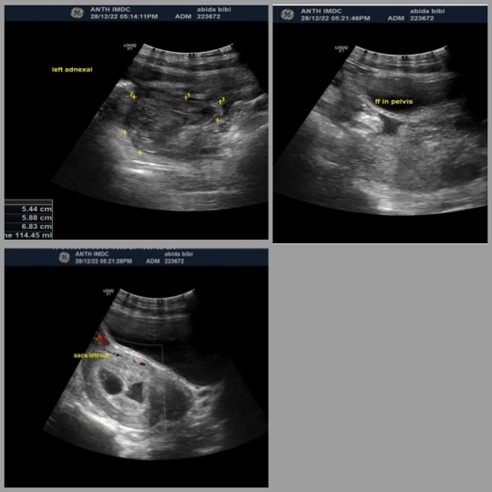
Figure 1: transabdominal ultrasound shows (A) left complex heterogeneous adnexal mass - intrauterine pregnancy of 6 weeks and 5 days (B) free fluid seen in the pelvis (C) intra-uterine gestational sac with fetal pole, cardiac activity positive, and pseudo gestational sac also present without fetal pole at the time of scan
On examination, her blood pressure was 100/60 mmHg, and her pulse rate was 90 bpm. Abdominal examination revealed tenderness in the left iliac fossa. She had no urinary complaints or vaginal bleeding. On admission, laboratory tests revealed a white blood cell count of 7780/mm3, a haematocrit of 34.4%, a serum haemoglobin concentration of 11.2 g/dL, and a platelet level of 263000/mm3. The serum-human chorionic gonadotropin (HCG) test was not performed. A trans-abdominal and trans-vaginal ultrasound revealed the following findings: A well-formed yet irregular gestational sac measuring 10.4mm in the left adnexal region and a fetal pole measuring 3.4mm within the gestational sac, indicating a gestational age of 6 weeks. No cardiac activity was observed in the fetal pole at the time of the scan. Moreover, a heterogeneous area with no internal vascularity surrounded the ectopic pregnancy, and there was evidence of mild free fluid with internal echoes in the pelvic cavity, suggesting a ruptured ectopic pregnancy in the left fallopian tube, adjacent phlegmon formation, and concomitant mild hemoperitoneum and peritonitis.
Additionally, an intrauterine gestational sac (6 weeks and 6 days) with a fetal pole of 6 weeks and 4 days, showing cardiac activity, was detected. An ill-defined anechoic area adjacent to the intrauterine gestational sac was also noted.
Treatment and Outcome: Abida Bibi was referred to the gynecology department and admitted for emergency laparotomy. The surgical findings confirmed the sonological observations: a left-sided ruptured ectopic pregnancy with hemoperitoneum. Both ovaries and the right fallopian tube were found to be healthy. The ruptured ectopic pregnancy was surgically removed.
The postoperative period was unremarkable, and a follow-up ultrasound was performed on December 30, 2022, showing a single, live intrauterine pregnancy of 6 weeks and no left adnexal mass. A subsequent ultrasound on January 7, 2023, revealed a bulky retroverted uterus with an intrauterine pregnancy of 7 weeks and 1 day, along with positive cardiac activity. Hyperechoic areas suggestive of peri-sac/sub-chorionic collection was also observed. The patient did not comply with recommended follow-up scans.
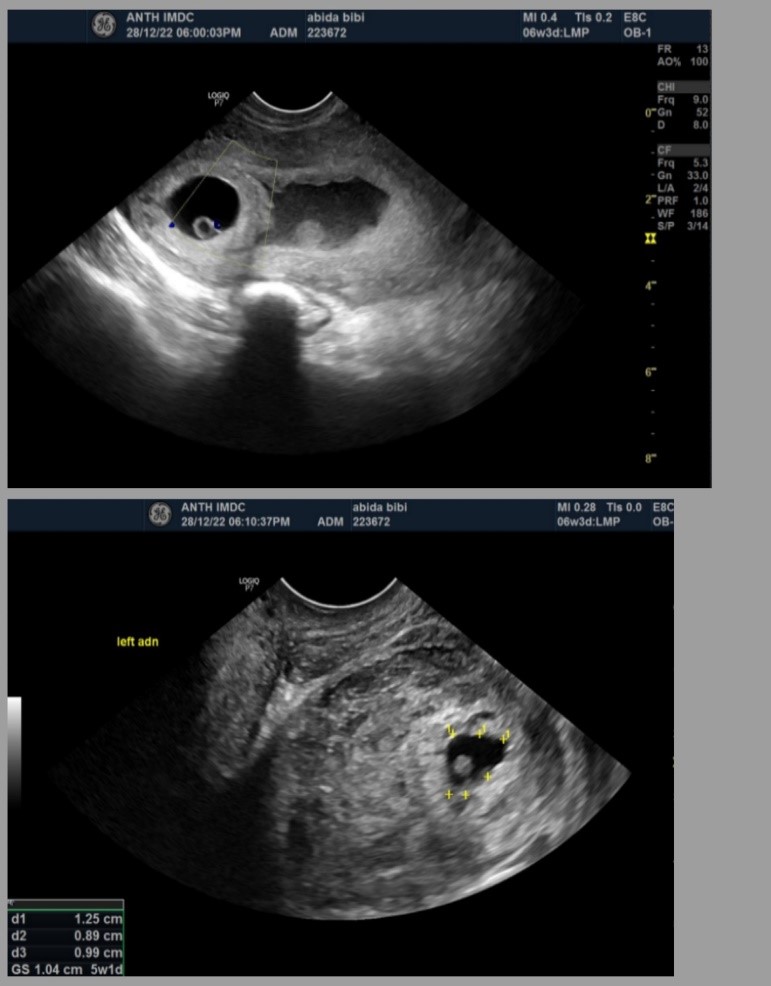
Figure 2: Transvaginal ultrasound shows (A) a well-formed intrauterine gestational sac with fetal pole and cardiac activity positive (B) left adnexal mass - well-defined gestational sac with fetal pole seen however cardiac activity negative
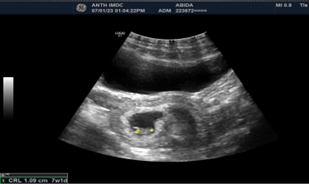
Figure 3: Bulky retroverted uterus with intrauterine pregnancy of 7w 1d with positive cardiac activity - hyperechoic areas likely to be peri-sac/sub-chorionic collection.
The rare type of multiple gestations is heterotrophic pregnancy with a combination of an extrauterine and intrauterine pregnancy.4 The HP incidence after spontaneous conception is 1 per 30,000 pregnancies; however, greater rates have been linked to ART such as stimulation of ovulation and IVF. Of the 553,577 births reported in the National ART Surveillance System between 2001 and 2011, only 485 heterotopic pregnancies—or 1 in 1111—were found.6 Our patients had a spontaneous conception with no history of ART or PID, which may have reduced her possibility of having a heterotrophic pregnancy. HP’s symptoms are not particular. In 24% of cases, HP may not cause any symptoms. The most common HP symptom is abdominal pain, while hypovolemic shock and vaginal bleeding are also frequent. Urgent medical attention is necessary when vaginal bleeding and hypovolemic shock occur, as they frequently signify an EP rupture.7 Our patient with a history of positive UPT and gestational amenorrhea, presented with a complaint of abdominal pain only, due to the lack of other symptoms a differential
diagnosis was challenging, and suspicion of heterotrophic pregnancy was unlikely. However, TVS was used o correctly diagnose HP, allowing for prompt treatment before serious repercussions developed. TVS Revealed free fluid intra-peritoneal, and the ectopic pregnancy was quickly identified as ruptured.2 It is difficult to diagnose HP early since an intrauterine embryo is observed in the US and a rising serum B-HCG level makes people assume it is a normal pregnancy, and very few people check for an EP if the patient is asymptomatic. When an intrauterine embryo is discovered, it is imperative to examine and document the uterine adnexa. The claimed sensitivity and specificity for identifying an EP in the US are 71–100% and 41–99%, respectively.7 Most HP cases are discovered after emergency
laparotomies due to tubal ruptures.5Expectant management, surgical management (either
laparoscopy or laparotomy), and sonography-guided embryo aspiration with or without embryo-
killing medications are all alternatives for treatment.7
The patient' s health, the size and location of an EP, prior pregnancies, the viability of both intrauterine and extrauterine gestation, and the medical personnel and #39; s experience all influence the course of treatment. Expectant care may be considered when a patient is symptom-free and the un-ruptured ectopic embryo has a limited
craniocaudal length, no cardiac activity, and a falling level of -HCG.8 Emergency surgery is strongly advised for individuals exhibiting unstable hemodynamics or exhibiting any other symptoms suggesting the rupture of an extra uterine pregnancy. Surgical therapy has the advantage of being able to remove an EP completely, however, there may be a larger chance of an IU embryo aborting.9 Considering sonological findings showing free fluid in the cul-de-sac, there was a possibility of ruptured EP, so an emergency laparotomy with left salpingectomy was
performed on our patient. Preserving both the ovaries and right fallopian tube is crucial for
young females who intend to have many children.
The IU embryo grew normally
throughout the successful postoperative phase. Approximately 60 to 70% of HP cases outcome
in live births with results comparable to singleton pregnancies.5
The prevalence of heterotopic pregnancy has risen in recent years, with the advent of medically assisted reproduction. Its occurrence in the spontaneous cycle is rare and might be fatal to the patient.4 Consider heterotopic pregnancy in the differential diagnosis of abdominal pain in a reproductive patient, with symptoms of ectopic pregnancy. In the absence of any predisposing risk factors, heterotopic pregnancy can occur. 10 To rule out the possibility of a heterotopic pregnancy, a thorough examination of the pelvis and adnexa should be performed in the US [10]. This case highlights the importance of early recognition, timely intervention, and close follow-up to ensure a favourable outcome for both intrauterine and ectopic pregnancies.
- Kajdy A, Muzyka-Placzyńska K, Filipecka-Tyczka D, Modzelewski J, Stańczyk M, Rabijewski M. A unique case of diagnosis of a heterotopic pregnancy at 26 weeks–case report and literature review. BMC Pregnancy and Childbirth. 2021 Dec;21:1-6. https://doi.org/10.1186/s12884-020-03465-y
- Chadee A, Rezai S, Kirby C, Chadwick E, Gottimukkala S, Hamaoui A, Stankovich V, Hale T, Gilak H, Momtaz M, Sasken H. Spontaneous heterotopic pregnancy: dual case report and review of the literature. Case Reports in Obstetrics and Gynecology. 2016 Jun 19;2016. https://doi.org/10.1155/2016/2145937 Kumar R, Dey M. Spontaneous heterotopic pregnancy with tubal rupture and pregnancy progressing to term. Medical journal armed forces India. 2015 Jul 1;71:S73-5. https://doi.org/10.1016%2Fj.mjafi.2013.02.017
- Perkins KM, Boulet SL, Kissin DM, Jamieson DJ, National ART Surveillance (NASS) Group. Risk of ectopic pregnancy associated with assisted reproductive technology in the United States, 2001–2011. Obstetrics and gynecology. 2015 Jan;125(1):70. https://doi.org/10.1097/aog.0000000000000584
- Černiauskaitė M, Vaigauskaitė B, Ramašauskaitė D, Šilkūnas M. Spontaneous heterotopic pregnancy: Case report and literature review. Medicina. 2020 Jul 22;56(8):365. https://doi.org/10.3390/medicina56080365 Baxi A, Kaushal M, Karmalkar HK, Sahu P, Kadhi P, Daval B. Successful expectant management of tubal heterotopic pregnancy. Journal of Human Reproductive Sciences. 2010 May;3(2):108. https://doi.org/10.4103%2F0974-1208.69333
- Li JB, Kong LZ, Yang JB, Niu G, Fan L, Huang JZ, Chen SQ. Management of heterotopic pregnancy: experience from 1 tertiary medical center. Medicine. 2016 Feb;95(5). https://doi.org/10.1097/md.0000000000002570 Mihmanli V, Kilickaya A, Cetinkaya N, Karahisar G, Uctas H. Spontaneous heterotopic pregnancy presenting with hemoperitoneum. The Journal of Emergency Medicine. 2016 Jan 1;50(1):44-6. https://doi.org/10.1155%2F2016%2F2145937.
![]()
An Official Publication of
Islamabad Medical & Dental College
Volume 12 Issue 4
Editorial
Address of Correspondence
Saba Khilji
Email:
saba.khilji5@gmail.com
Cite this article.Khilji S, Anum W, Tbassum M, Tahir A, Niazi M, Naeemah. A Unique Case Report of Heterotopic Pregnancy. J Islamabad Med Dental Coll. 2023; 12(4): 360-364. DOI: https://doi.org/10.35787/jimdc.v11i4.1069