Distribution of Extended-spectrum β-lactamase and Metallo-β-lactamase-producing Pseudomonas aeruginosa in Tertiary Care Hospitals of Lahore, Pakistan
Syeda Aneela 1, Noor-ul-Ain, 2, Samyyia Abrar 3, Muhammad Seed 4, Shahida Hussain 5, Abdul Hannan 6, Saba Riaz 7
1-3, 5 Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore.
4 DHQ Hospital Mandi Bahauddin, Primary & Secondary Health Care Department, Government of Punjab, Pakistan.
6 Professor, Department of Microbiology, University of Health Sciences, Lahore († Deceased).
7 Assistant Professor, Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore
Background: Pseudomonas aeruginosa (P. aeruginosa) is an important bacterial pathogen most frequently associated with nosocomial infections, especially in immuno-compromised patients. Early detection of these life threatening, β-lactamase producing bacteria is essential to aid infection control and to prevent their dissemination. The aim of our study was to detect the presence of Extended-Spectrum β-Lactamase (ESBL) and Metallo-β-Lactamase (MBL) strains of Pseudomonas aeruginosa.
Material and Methods: Eighty-eight identified strains of P. aeruginosa were collected from Chughtai Laboratories, Combined Military Hospital and Children Hospital, Lahore. These strains were sub-cultured and after confirming the cultural characteristics by Gram staining and colony morphology, manual biochemical identification was done. Susceptibility to various antibiotics and production of extended-spectrum β-lactamases (ESBLs) and metallo-β-lactamases (MBLs) were determined using modified Kirby Bauer disk diffusion method, double disk synergy test, combined disk synergy test (CDST) and inhibitor-potentiated disk diffusion test (IPD) respectively.
Results: Out of eighty-eight strains tested, three were ESBL producers (3.4%) and eleven strains (12.5%) were found to be resistant to carbapenems. Of these, eight were MBL producers (72.7%). All these β-lactamase producing strains (14 strains) were multidrug-resistant (MDR). Piperacillin and piperacillin/tazobactam proved to be the most effective antibiotics in both types of β-lactamase producing strains.
Conclusion: Our study shows noticeable emergence of β-lactamases (ESBLs & MBLs) in P. aeruginosa. All of these strains were MDR. It reveals a correlation of these β-lactamases with multidrug resistant genes.
Key words: ESBL, MBL, MDR. Pseudomonas aeruginosa, Pakistan, DDST, CDST, IPD
Pseudomonas aeruginosa is an important opportunistic pathogen responsible for various healthcare associated infections like pneumonia, sepsis, wounds and urinary tract infections.1,2 This organism can cause deadly infections and is most commonly isolated from wound infections in developing countries3,4. It is professed to be associated with high mortality rate i.e. up to 61%.5 Carbapenems are most effective antibiotics against several pseudomonal infections. However resistance to this innovative antibiotic has been observed in recent years6 Metallo β-lactamase is usually associated with carbapenems-resistance in P. aeruginosa.7 MBL hydrolyzes most of the β-lactam antibiotics except monobactams. Additionally, these enzymes are resistant to most of the β-lactam inhibitors like clavulanic acid, sulbactam.8 Moreover, MBL-producing P. aeruginosa are responsible for high a mortality rate9.
Pseudomonal infections are often burdensome because of an intrinsic and acquired resistance of the organism to common antimicrobials, eventually resulting in emergence of multidrug resistant strains of P. aeruginosa.10 Among these different resistant mechanisms, β-lactamases including Extended-Spectrum β-Lactamases and Metallo β-Lactamases are predominantly observed in P. aeruginosa.11 ESBL hydrolyzes β-lactam drugs like cefotaxime, ceftriaxone, ceftazidime and monobactams with no efficacy on cephamycins and carbapenems. β-lactamase inhibitors like clavulanic acid are effective against these enzymes8,12.
The aim of this research was to identify ESBL and MBL-producing P. aeruginosa and to determine the antimicrobial susceptibility patterns of these strains (ESBL and MBL producing P. aeruginosa).
The study was conducted at Department of Microbiology, University of Health Sciences, Lahore. This was an observational, cross-sectional study conducted over a duration of one year from October 2008 to October 2009. Eighty-eight strains of P. aeruginosa were collected from Chughtai Lahore Laboratories, Combined Military Hospital, Lahore and Children Hospital, Lahore. These strains were isolated in these laboratories from wound swabs, pus, bronchial washings and blood. Identified strains of P. aeruginosa were sub-cultured in Department of Microbiology, University of Health Sciences, Lahore. After confirming the cultural characteristics by Gram staining and colony morphology, manual biochemical identification was done by API 20NE identification system (BioMerieux, France). Bio-statistical analysis was done by Pearson’s chi-square test as previously used by Giriyapur et al13 .
Antimicrobial susceptibility of P.aeruginosa was performed using Mueller-Hinton agar (Oxoid UK), according to Clinical Laboratory Standards Institute (CLSI, 2009) guidelines. Antibiogram profile was generated by using: amoxicillin/clavulanic acid (30𝜇g), ceftriaxone (30𝜇g), ceftazidime (30𝜇g), ciprofloxacin (5𝜇g), sulfamethoxazole/trimethoprim (25𝜇g), piperacillin (100𝜇g), piperacillin/tazobactam (100\10𝜇g), aztreonam (30𝜇g), meropenem (10𝜇g), imipenem (10𝜇g), and amikacin (30𝜇g). Amoxicillin/clavulanic acid was used for screening of ESBL producers and sulfamethoxazole/trimethoprim (SXT 5𝜇g) were used to check whether it is effective in β-lactamase producers (Figure 1).
ESBL production in all the isolates was detected by double disc synergy test (DDST) as described byJarlier et al14. Synergistic effect of amoxicillin + clavulanic acid (20 + 10 μg) was checked with ceftazidime (30 μg) and ceftriaxone (30 μg). Strains indicating >5mm synergistic zone were confirmed as ESBLproducers.15
MBL production in the carbapenem-resistant isolates was detected following two methods. Pseudomonas aeruginosa and Enterobacter cloacae positive for MBL were used as positive control. For combination disc test (CDST), imipenem (10 µg) and meropenem (10 µg) discs (Oxoid) alone and in combination with 0.5 M EDTA were used. Increase in the inhibition zone of ≥ 7mm by the addition of EDTA indicates MBL-production.16 For Inhibitor potentiated disk diffusion test (IPD), imipenem (10 µg) (Oxoid) was used along with disc of 0.5 EDTA solution. Presence of an augmentation zone (clearing zone) i.e. >7mm between EDTA and imipenem discs was interpreted as being positive test.17
Antimicrobial susceptibility pattern of P. aeruginosa strains (Table I) showed piperacillin/tazobactam as the most sensitive antibiotic with 95.5% susceptible isolates. Piperacillin (94.3%) was second most sensitive antibiotic. There was no significant difference between these two antibiotics. It was followed by meropenem (89.8%), imipenem (87.5%), amikacin (84.1%), ceftazidime (80.7%), aztreonam (71.6%), and ciprofloxacin (69.3%). Ceftriaxone was least effective among β- lactams with only 29.5% susceptible isolates. Amoxicillin/clavulanic acid and co-trimoxazole were resistant in all isolates (Figure 1).
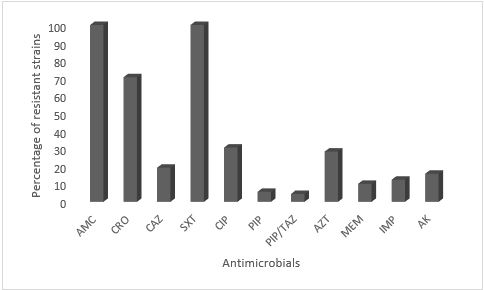
Figure 1: Antimicrobial resistance pattern of P. aeruginosa strains (n=88). Here, AMC =amoxicillin/calvulonic acid, CRO =ceftriaxone, CAZ =Ceftazidime, SXT=sulphamethoxazole/trimethoprim, ATM aztreonam, AK =Amikacin, CIP = ciprofloxacin, PRL= piperacillin, TZP=piperacillin/tazobactam, IPM=imipenem and MEM= Meropenem.
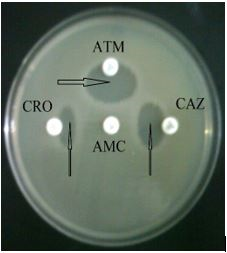
Figure 2: Demonstration of ESBL phenomenon by Double Disc Synergy test (DDST)
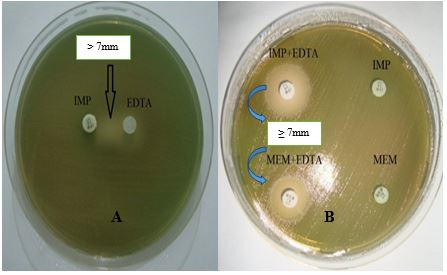
Figure 3: MBL detection tests. A) Combined Disk Synergy Test and B) Inhibitor Potentiated Disk Diffusion
Table: I. Antimicrobial susceptibility pattern of P. aeruginosa isolates (n=88) |
|||||
Sr. |
Antimicrobials |
NS |
S (%) |
NR |
R (%) |
1 |
Co-amoxiclav |
0 |
0 |
88 |
100 |
2 |
Ceftriaxone |
26 |
29.5 |
62 |
70.5 |
3 |
Ceftazidime |
71 |
80.7 |
17 |
19.3 |
4 |
Cotrimoxazole |
0 |
0 |
88 |
100 |
5 |
Ciprofloxacin |
61 |
69.3 |
27 |
30.7 |
6 |
Piperacillin |
83 |
94.3 |
5 |
5.7 |
7 |
Piperacillin/tazobactam |
84 |
95.5 |
4 |
4.5 |
8 |
Aztreonam |
63 |
71.6 |
25 |
28.4 |
9 |
Meropenem |
79 |
89.8 |
9 |
10.2 |
10 |
Imipenem |
77 |
87.5 |
11 |
12.5 |
11 |
Amikacin |
74 |
84.1 |
14 |
15.9 |
- n =Total number of strains
- NS=number of sensitive strains
- NR= number of resistant strains
- S (%) = percentage of sensitive strains
- R (%) = percentage of Resistant strains
Table II: Antimicrobial resistance pattern of ESBL and MBL-producing strains of Pseudomonas aeruginosa |
|||||
Sr. No |
Antibiotics |
ENR |
E (%) R |
MNR |
M (%) R |
1. |
Co-amoxiclav |
3 |
100 |
8 |
100 |
2. |
Ceftriaxone |
3 |
100 |
8 |
100 |
3. |
Ceftazidime |
3 |
100 |
8 |
100 |
4. |
Cotrimoxazole |
3 |
100 |
8 |
100 |
5. |
Ciprofloxacin |
3 |
100 |
8 |
100 |
6. |
Piperacillin |
0 |
0.0 |
0 |
0.0 |
7. |
Piperacillin/tazobactam |
0 |
0.0 |
0 |
0.0 |
8. |
Aztreonam |
3 |
100 |
6 |
75 |
9. |
Meropenem |
0 |
0.0 |
8 |
100 |
10. |
Imipenem |
0 |
0.0 |
8 |
100 |
11. |
Amikacin |
2 |
66.6 |
8 |
100 |
- ENR= number of resistant strains among ESBL producers
- E (%) R = percentageof resistant strains among ESBL producers
- MNR=number of resistant strains among MBL producers
- M (%) R =percentageof resistant strains among MBL producers
Out of 88 cultured isolates of P. aeruginosa three (3.4%) were ESBL-producers and eleven strains (12.5%) were resistant to carbapenems of which eight (72.7%) were MBL-producers. All the ESBL and MBL-producing strains were found to be MDR. ESBLs were resistant to β-lactam antibiotics except carbapenems where 100% susceptibility towards these antibiotics was observed. Moreover, ESBLs also indicated high susceptibility towards amikacin (Table II). MBL-producers indicated 100% resistance towards applied antibiotics except piperacillin and piperacillin /tazobactam combination where 100% sensitivity was observed (Table III).
Table III. Antimicrobial susceptibility pattern of MBL-producing and Non-producing Isolates |
|||||||
Antimicrobials |
MBL Producing |
MBL Non-producing |
X2 |
||||
R |
S |
S (%) |
R |
S |
S (%) |
P Value |
|
Co-amoxiclav |
8 |
0 |
0.0 |
80 |
0 |
0.0 |
* |
Ceftriaxone |
8 |
0 |
0.0 |
54 |
26 |
29.5 |
0.05 |
Ceftazidime |
8 |
0 |
0.0 |
09 |
71 |
80.7 |
0.00 |
Cotrimoxazole |
8 |
0 |
0.0 |
80 |
0 |
0.0 |
* |
Ciprofloxacin |
8 |
0 |
0.0 |
19 |
61 |
69.3 |
0.00 |
Piperacillin |
0 |
8 |
100 |
05 |
75 |
94.3 |
0.467 |
Piperacillin/ |
0 |
8 |
100 |
04 |
76 |
95.5 |
0.517 |
Aztreonam |
6 |
2 |
25 |
19 |
61 |
71.6 |
0.02 |
Meropenem |
8 |
0 |
0.0 |
01 |
79 |
89.8 |
0.00 |
Imipenem |
8 |
0 |
0.0 |
03 |
77 |
87.5 |
0.00 |
Amikacin |
8 |
0 |
0.0 |
06 |
74 |
84.1 |
0.00 |
- n =Total number of strains
- R= Resistant
- S= Sensitive
- * = no statistics is computed as AMC and SXT are constant (Resistant in all isolates).
- P value < 0.05 = significant difference
P. aeruginosa is an important nosocomial pathogen, endowed with a variety of resistance mechanisms that may cause multidrug or even pan-drug resistance. Extended-spectrum β-lactamases (ESBLs) and carbapenemases (MBLs) are among the most common causative agents.18 In the present study, three strains (3.5%) were ESBL producers detected by the double disc synergy test which is supported by the results of Kotwal et al in which 6% of ESBL were detected among cefepime resistant P. aeruginos.19,20 While the findings of Wolska and Jakubczak, (2008) showed no ESBL detection in P. aeruginosa isolates.21 However, it is in contrast to the study conducted in Pakistan, where 35.8% strains of P.aeruginosa were ESBL-producers.22 This disparity might be due to the evidence that more MDRs are isolated from burn unit.23
In the present study eleven strains (12.5%) of P. aeruginosa indicated resistance to carbapenems of which eight were detected as MBL-producers by using the CDST and IPD methods. Our data indicates that frequency of MBL-producing strains among imipenem resistant P. aeruginosa is 72.7%. While Irfan et al reported 100% of MBL-production among carbapenem resistant P. aeruginosa.24 Our study results are similar to the findings of Kali et al where 72.7% MBL-producers among carbapenem-resistant P. aeruginosa isolates were observed.25 A recent study in Pakistan has described the incidence of ESBL and MBL in clinical isolates of MDR P. aeruginosa as 23.94% and 40.84% respectively.26
Our data showed increased resistance to commonly used antibiotics. Piperacillin/tazobactam and piperacillin alone proved to be effective antibiotics. Carbapenems were found to be the second most effective antibiotic group accounting for 12.5% and 10.2% resistance for imipenem and meropenem respectively, which is consistent with national antibiotic resistance data of Pakistan in 2009.27
The β-lactamase-producers were resistant to all other antibiotics except the above-mentioned ones, so there was a narrow range for a suitable drug of choice. P. aeruginosa had shown an increased resistance to the fluoroquinolone (30.7%). Resistance rates of amikacin, ceftazidime and aztreonam remained 15.9%, 19.3%, 28.4% respectively and similar reports of 22%, 30% and 19% resistance have been reported by Pakistan Antimicrobial Resistance Network (PARN). Ceftriaxone was least effective among β-lactams with only 29.5% susceptible isolates. All isolates were resistant to amoxicillin/clavulanic acid and co-trimoxazole (as already established). These values are comparable to the findings available in Pakistan that are 83.8% and 79.24% resistance respectively.22 There were 14 (15.9%) isolates as MDR, three of these were ESBL and eight out of twelve carbapenem resistant isolates were MBL-producers. This is an alarming sign as few therapeutic options are left for the patients infected with these strains.
Early screening of P. aeruginosa isolates to detect ESBL and MBL-production should be emphasized. Therefore, routine testing of the isolates of P. aeruginosa for sensitivity to ceftazidime, cefotaxime and carbapenems may represent a cost-effective way for screening of ESBLs and MBLs. Our study has introduced an easy and cost-effective inhibitor potentiated disk diffusion (IPD) method for MBL detection in Pakistan. Thus, double disk synergy test and combined disk synergy test (CDST) / inhibitor-potentiated disk diffusion method (IPD) can easily be used to confirm the ESBL and MBL phenotypically.
The emergence of these β-lactamases along with MDR genes in P. aeruginosa may adversely muddle the clinical management of such patients. High frequency of these enzymes urges the infection control teams of hospitals to design some preventive measures to stop the dissemination of these resistant strains.
Our study shows noticeable emergence of these β-lactamases in P. aeruginosa. All of these strains were MDR. It reveals a correlation of these β-lactamases with multidrug resistant genes.
- Jefferies J, Cooper T, Yam T, Clarke S: Pseudomonas aeruginosa outbreaks in the neonatal intensive care unit–a systematic review of risk factors and environmental sources. J. Med. Microbiol 2012, 61(8):1052-1061.
- Lister PD, Wolter DJ, Hanson ND: Antibacterial-resistant Pseudomonas aeruginosa: clinical impact and complex regulation of chromosomally encoded resistance mechanisms. J. Clin. Microbiol Reviews 2009, 22(4):582-610.
- Rahbar M: Laboratory Evaluation of Iranian Commercially Provided Antibiotic Disks With Conventional E-Test for Susceptibility Testing in Three Most Isolated Multi-drug Resistant Organisms. Internet J Microbiol 2008, 5(1).
- Aguila LA, Lopes MRU, Pretti FZ, Sampaio-Barros PD, de Souza FHC et al. Clinical and laboratory features of overlap syndromes of idiopathic inflammatory myopathies associated with systemic lupus erythematosus, systemic sclerosis, or rheumatoid arthritis. Int J Clin Rheumtol 2014, 33(8):1093-1098.
- Bassetti M, Righi E, Viscoli C: Pseudomonas aeruginosa serious infections: mono or combination antimicrobial therapy? Curr Med Chem 2008, 15(5):517-522.
- Hammami S, Boubaker IB-B, Ghozzi R, Saidani M, Amine S, Redjeb SB: Nosocomial outbreak of imipenem-resistant Pseudomonas aeruginosa producing VIM-2 metallo-β-lactamase in a kidney transplantation unit. Diagn pathol 2011, 6(1):106.
- Franklin C, Liolios L, Peleg AY: Phenotypic detection of carbapenem-susceptible metallo-β-lactamase-producing gram-negative bacilli in the clinical laboratory. J. Clin. Microbiol 2006, 44(9):3139-3144.
- Bush K, Jacoby GA, Medeiros AA: A functional classification scheme for beta-lactamases and its correlation with molecular structure. Antimicrob. Agents Chemother 1995, 39(6):1211.
- Zavascki AP, Barth AL, Gonçalves ALS, Moro ALD et al. The influence of metallo-β-lactamase production on mortality in nosocomial Pseudomonas aeruginosa infections. J Antimicrob Chemother 2006, 58(2):387-392.
- Strateva T, Yordanov D: Pseudomonas aeruginosa–a phenomenon of bacterial resistance. J. Med. Microbiol 2009, 58(9):1133-1148.
- Rafiee R, Eftekhar F, Tabatabaei SA, Tehrani DM: Prevalence of extended-spectrum and metallo β-lactamase production in AmpC β-lactamase producing Pseudomonas aeruginosa isolates from burns. undishapur J.Microbiol 2014, 7(9).
- Paterson DL, Bonomo RA: Extended-spectrum β-lactamases: a clinical update. J. Clin. Microbiol Reviews 2005, 18(4):657-686.
- Giriyapur RS, Nandihal NW, Krishna B, Patil AB, Chandrasekhar M: Comparison of disc diffusion methods for the detection of extended-spectrum Beta lactamase-producing enterobacteriaceae. J lab physicians 2011, 3(1):33.
- Jarlier V, Nicolas M-H, Fournier G, Philippon A: Extended broad-spectrum β-lactamases conferring transferable resistance to newer β-lactam agents in Enterobacteriaceae: hospital prevalence and susceptibility patterns. Clin Infect Dis 1988, 10(4):867-878.
- Abrar S, Vajeeha A, Ul-Ain N, Riaz S: Distribution of CTX-M group I and group III β-lactamases produced by Escherichia coli and klebsiella pneumoniae in Lahore, Pakistan. Microb Pathog 2017, 103:8-12.
- Yong D, Lee K, Yum JH, Shin HB, Rossolini GM, Chong Y: Imipenem-EDTA disk method for differentiation of metallo-β-lactamase-producing clinical isolates of Pseudomonas spp. and Acinetobacter spp. J. Clin. Microbiol 2002, 40(10):3798-3801.
- Oh E-J, Lee S, Park Y-J, Park JJ, Park K, Kim S-I et al. Prevalence of metallo-β-lactamase among Pseudomonas aeruginosa and Acinetobacter baumannii in a Korean university hospital and comparison of screening methods for detecting metallo-β-lactamase. J Microbiol Methods 2003, 54(3):411-418.
- Potron A, Poirel L, Nordmann P: Emerging broad-spectrum resistance in Pseudomonas aeruginosa and Acinetobacter baumannii: mechanisms and epidemiology. Int J Antimicrob Agents 2015, 45(6):568-585.
- Wang R, Zeng YL, Qin HM, Lu YL, Huang HT, Lei M et al. Association of interleukin 22 gene polymorphisms and serum IL‐22 level with risk of systemic lupus erythematosus in a Chinese population. Clin. Exp. Immunol 2018; 193(2):143-51
- Kotwal A, Biswas D, Kakati B, Singh M: ESBL and MBL in cefepime resistant Pseudomonas aeruginosa: an update from a rural area in Northern India. J Clin Diagn Res: JCDR 2016, 10(4):DC09.
- Wolska K, Jakubczak A, Soszyńska A: Antibiotic susceptibility and occurrence of ESBL, IBL and MBL in Pseudomonas aeruginosa strains. Med Dosw Mikrobiol 2008, 60(2):111-119.
- Ullah F, Malik SA, Ahmed J: Antimicrobial susceptibility and ESBL prevalence in Pseudomonas aeruginosa isolated from burn patients in the North West of Pakistan. Burns 2009, 35(7):1020-1025.
- Al-jashamy K, Bhuiyan M, Sabet NS: ESBL and MBL genes detection and plasmid profile analysis from Pseudomonas aeruginosa clinical isolates from Selayang Hospital, Malaysia. Blood, 6:11.12.
- Irfan S, Zafar A, Guhar D, Ahsan T, Hasan R: Metallo-β-lactamase-producing clinical isolates of Acinetobacter species and Pseudomonas aeruginosa from intensive care unit patients of a tertiary care hospital. Indian J Med Microbiol 2008, 26(3):243.
- Kali A, Srirangaraj S, Kumar S, Divya HA, Kalyani A, Umadevi S: Detection of metallo-beta-lactamase producing Pseudomonas aeruginosa in intensive care units. Australas Med J 2013, 6(12):686.
- Ullah W, Qasim M, Rahman H, Khan S, ur Rehman Z, Ali N et al. CTX-M-15 and OXA-10 beta lactamases in multi drug resistant Pseudomonas aeruginosa: First report from Pakistan. Microb Pathog 2017, 105:240-244.
- http://parn.org.pk