A Huge Lipoma Involving Left Cheek Region: A Case Report
Muhammad Jamal1 , Kaleem Ullah 2, Laiba Saher3
1 AssistantProfessor,Department ofOral and Maxillofacial Surgery, Islamabad Medical and Dental College
2 Consultant, Department of Oral and Maxillofacial Surgery, KRL Hospital, Islamabad
3 Postgraduate Resident, Department of Oral and Maxillofacial Surgery, Islamabad Medical and Dental College
Lipomas are very common benign lumps that can be encountered in any part of the body but a small proportion present in the head and neck region. In this case reportwe have discussed the diagnosis and surgical treatment of an asymptomatic huge lipoma of left cheek. The patient had this swelling present for the last 5 years. Initially there was a slight increase in the size of the swelling but since the last 3 years there is no change in size. There wasno history of associated pain and tenderness. The patient had esthetic concerns because of which the lesion was excised. These lipomas continue to grow slowly, showing variable signs including dysphagia, dyspnea, and dysphonia due to the compressing effect on surrounding structures. It can also be a matter of cosmetic concern. With this case report, authors will alsohighlight the diagnostic modalities and treatment for lipomas occurring in unusual areas in the body. It is a rare finding that occurs anterior to parotidbut can be treated successfully by current surgical approach.
Key Words:Cheek Swelling, Esthetics, Lipoma
In head and neck region,lipoma is one of the most common forms of benign neoplasm arising mostly in the posterior cervical triangle of the neck. It can occur in and around the parotid gland or the parapharyngeal space in the head and neck territory. Presence of a lipoma should be included in the differential diagnosis of swellings of parotid gland. A thorough preoperative clinical, radiological and cytological examination should be performed to further investigate the swelling.
A 42 years old male patient reported toOral & Maxillofacial Surgeryclinic with a cheek swelling on the left side of face since last 5 years. Initially there was a slight increase in the size of swelling but for the partlast 3 years, there was no change in size. There was no history of associated pain and tenderness. The patient wanted removal of the lesion for esthetic reasons.
On clinical examination there was localized, mobile, firm swelling involving the left cheek region,measuring approximately 3x3 cm in size.(Figure 1)The overlying skin was of normal color and texture and not fixed to the lesion. There was no associated neurological deficit. Ultrasound examination revealed well defined hyper echoic area measuring 1.8x1.6 cm in size, suggestive of lipoma. Color Doppler ultrasound revealed normal blood flow in the area with normal adjacent structures. Fine needle aspiration cytology (FNAC) showed hemorrhage, fused stromal cells and lipocytes.
CT scan revealed a well-defined hypodense oval lesion on the left side of the face, just anterior to, but distinctly separate from the left parotid gland. The lesion measured 4.6x3.3 cm and had diffuse fat density. There was no mass affect due to the lesion on the surrounding structures. The CT findings were suggestive of a lipoma lying anterior to left parotid gland(Figure 2).
The patient was informed about the lesion and was advised for excision under general anesthesia (GA). Under aseptic measures and standard surgery protocol, extended sub-mandibular incision was made 2cm below the lower border of the left mandible and dissection performed in the sub-platysmal plane to prevent damage to marginal mandibular branch of facial nerve. (Figure 3) The lesion was dissected from the surrounding tissue without damaging the parotid fascia and was removed.Hemostasis was achieved and the wound was closed using 3/0 vicryl while the skin incision was closed using 3/0 proline. The excised specimen was sent for histopathological examination.
The patient was examined post operatively for any neurological deficit, which was not present. Histopathology report confirmed the diagnosis of lipoma in the left cheek region measuring 5x5x3 cmin dimensions. On follow-up visits, no neurological deficit was noted and the wound healed satisfactorily without any post-operative complaint

Figure 1: Preoperative Pictures showing left cheek swelling
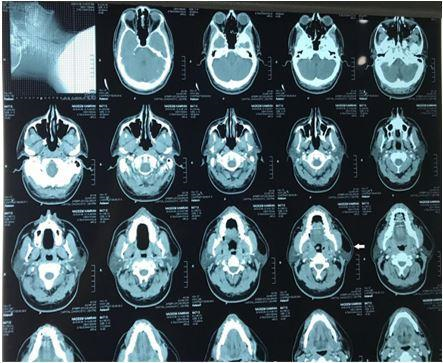
Figure 2: Axial view of a pre-operative CT scan showing a well defined hypo-dense
oval lesion just anterior to the left parotid gland
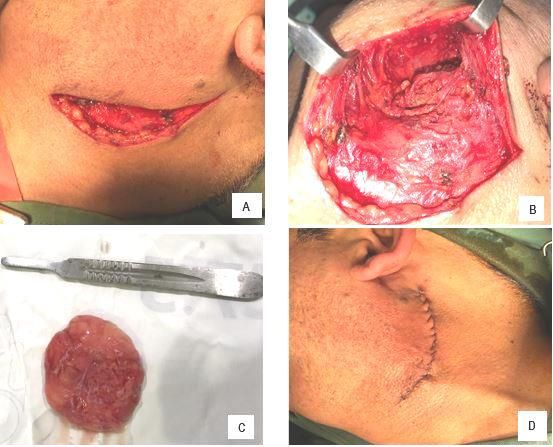
Figure 3: Extended submandibular incision during surgery (A), exposure and removal of the lesion (B),
excised lipoma (C), and surgical incision closed with sutures (D)
Lipoma, the most common benign mesenchymal neoplasm of soft tissue (15–20%), account for only 1–4% of all neoplasms arising in the oral cavity. Roux in 1848 gave details of an oral lipoma for the first time, and named it as a “yellow epulis”.1 Lipomas are most common in fifth to the sixth decades of life and males are more affected than females.2
Heredity, obesity, diabetes, radiation, endocrine disorders, insulin injection, corticosteroid therapy and trauma are among the multiple causes of lipoma. Trauma leads to formation of hematoma and lymphatic effusion and fat necrosis which results in lipoma formation.3 Lipomas are present in the subcutaneous tissues where they grow slowly. They are nearly always benign masses of adipose tissue arranged in lobules and many times have a fibrous capsule.4 Lipomas can be singular or multiple and are asymptomatic, unless they are large in size and compressing neurovascular structures. Large lipoma can lead to facial asymmetry and aesthetic consequences besides exerting pressure on surrounding structures.5
Lipomas are classified into multiple types namely simple lipoma, fibrolipoma, chondroid lipoma, myxolipoma, angiolipoma, angiomyolipoma, spindle cell lipoma,myelolipoma, sialolipoma, pleomorphic lipoma and atypical lipoma.6
Diagnostic imaging like ultrasonography, CT scan or MRI have an important role in diagnosing lipomas. Benign lipomas in CT scan images appear as hypoattenuated homogeneous masses without contrast enhancement, while in MRI images they tend to have high signal intensity in T1-weighted images with progressive decrease in signal intensity in T2-weighting.7 It has been shown by several studies that FNAC also aids in diagnosis of lipoma.8,9 Elliptical mass parallel to the skin surface that is hyper echoic relative to adjacent muscle and that contains linear echogenic lines at right angles to the ultrasound beam is appreciated on a sonogram.10
Treatment of choice of lipomas is definitely surgical excision. Surgery is opted for esthetic reasons, pressure symptoms due to enlarged size and malignancy. Recurrence occurs commonly so proper excision is required to prevent incomplete removal of this lesion.5
An appropriate clinical evaluation can lead to a diagnosis of lipoma. It is a rare finding that occurs anterior to parotid but can be treated successfully by current surgical approach.
- Kaur R, Kler S, Bhullar A. Intraoral lipoma: report of 3 cases. Dental Res J. 2011; 8(1): 48. PMID: 22132015
- Paparo F, Massarelli M, Giuliani G. A rare case of parotid gland lipoma arising from the deep lobe of the parotid gland. Ann Maxillofac Surg. 2016; 6(2): 308. doi: 10.4103/2231-0746.200335
- Dispenza F, De Stefano A, Romano G, Mazzoni A. Post-traumatic lipoma of the parotid gland: case report. ACTA Otorhinolaryngol Ital. 2008; 28(2): 87. PMID: 18669074
- El-Monem MH, Gaafar AH, Magdy EA. Lipomas of the head and neck: presentation variability and diagnostic work-up. J Laryngol Otol. 2006; 120(1): 47-55. doi: 10.1017/S0022215105004597
- Rana D, Raychaudhuri S, Arora S. A case of lipoma in lateral anterior neck: a common entity at an uncommon location. Int J Sci Rep .2017; 3(6):182-4. doi: 10.18203/issn.2454-2156
- Sathyaki DC, Roy MS.Lipomas of head and neck. Int J Otorhinolaryngol Head Neck Surg. 2018; 4(2): 368-71. doi: 10.18203/issn.2454-5929.ijohns20180521
- Najaf Y, Cartier C, Favier V, Garrel R. Symptomatic head and neck lipomas. Eur Ann Otorhinol Head Neck Ds. 2019; 136(2): 127-9. doi: 10.1016/j.anorl.2018.12.0013
- Fakhry N, Michel J, Varoquaux A, Antonini F, Santini L, Lagier A. et al. Is surgical excision of lipomas arising from the parotid gland systematically required? Eur Arch Oto-Rhino-L. 2012; 269(7):1839-44. doi: 10.1007/s00405-011-1843-0.
- Demir D, Eraslan Ö, Güven M, Kösem M. Rare cases of benign tumors of the head and neck: lipoma of larynx and sternocleidomastoid muscle. Kulak Burun Bogaz Ihtis Derg. 2016; 26(2):118-22. doi: 10.5606/kbbihtisas.2016.92155
- Ahuja AT, King AD, Kew J, King W, Metreweli C. Head and neck lipomas: sonographic appearance. Am J Neuroradiol. 1998;19(3):505-8.PMID:9541308.