Mandibular Reconstruction with Free Fibula Flap: Experience at Hayatabad Medical Complex, Peshawar
Syed Asif Shah1, Irfanullah2, Muhammad Bilal2, Mohammad Hamayun Shinwari2, Adeeba Ahmad3, Ehsanullah3
1 Associate Professor, Plastic Surgery Unit, Hayatabad Medical Complex, Peshawar
2 Assistant Professor, Plastic Surgery Unit, Hayatabad Medical Complex, Peshawar
3 Junior Registrar, Plastic Surgery Unit, Hayatabad Medical Complex, Peshawar
Background: Mandibular defects may result from trauma, infections, cancer ablation or radiation necrosis. These defects may vary according to the content and nature of the tissues that require reconstruction. The objective of this study was t o evaluate the outcome of vascularised free fibula flap for mandibular reconstruction in terms of flap success rate and complications.
Material and Methods: This prospective clinical study was carried out at Department of Plastic Surgery, Hayatabad Medical Complex, Peshawar from January 2014 to December 2018. The study included patients of either gender who underwent mandibular reconstruction with free fibula oseteocutaneous flap during the study period. Diabetic patients with underlying vascular pathologies and cachectic patients were excluded from the study.
Results: There were 56 patients with 38 males and 18 females. Their age ranged from 24-66 years with a mean age of 36 years. The mandibular defects resulted from various etiologies and included: Squamous cell carcinoma (n=27, 48.21%), Giant cell granuloma (n=3; 5.35%), Ameloblastoma (n=2; 3.57%), Road traffic accidents (n=10; 17.85%), Firearm injury (n=9; 16%), Bomb blast injury (n=3; 5.35%) and osteoradionecrosis (n=2; 3.57%). Primary reconstruction of the mandibular defects was performed in 44 patients, whereas delayed reconstruction was performed in 12 patients. Out of the 56 flaps, 49 flaps survived completely. Our share of complications was as follows: Wound infections (n=13; 23.21%), Skin graft loss at donor site (n=5; 8.95%), Complete flap loss (n=4; 7.14%), Orocutaneous fistulae (n=3; 5.35%), Ankle instability (n=2; 3.57%), Skin paddle necrosis (n=1; 1.78%) and sensory deficit distal to donor site (n=1; 1.78%).
Conclusions: Microvascular free fibula is a reliable tool for mandibular reconstruction following tumor resection or trauma. The flap has a high success rate and relatively fewer complications.
Key words: Mandibular defects, Mandibular reconstruction, Oseteocutaneous flap
Mandibular defects may result from trauma, infections, cancer ablation or radiation necrosis. These defects may vary according to the content and nature of the tissues that require reconstruction. Sometimes the defects are simple and may require a single type of tissue to be restored; for instance, isolated bony defects. But at times complex defects may need reconstruction of multiple tissues, such as bone and soft tissues. In either case, the reconstructive surgeon faces a challenge to restore the anatomic, functional and aesthetic aspects of the damaged structures.1,2 Trauma to facial region can result in distortion of anatomy and aesthetics of the region. The reconstruction of such defects and restoration to normal anatomy and function poses a challenge to the reconstructive surgeon. The facial region has certain discriminations in the structure of each anatomical part and it varies with individual patient. Each case is different from the other and requires individual consideration for proper management. Certain procedures have been adopted for reconstruction of various simple and complex defects of facial region. In the last three to four decades, microsurgical techniques have emerged as the standard techniques for the reconstruction of head and neck defects. Vascularized free fibula has emerged as the workhorse flap in this regard.3,4
Before the era of microvascular free tissue transfer, mandibular defects used to be reconstructed with metallic plates, free bone grafts or combination of both. Reconstruction with metallic plates resulted in complications like plate exposure, infection, plate fracture and insufficient facial symmetry.4,5 A number of microvascular free flaps were invented for reconstruction of mandible but each has its limitations. Free radial forearm flap was successfully employed wherein 10-12 cm of radius could be harvested for bone reconstruction. Its frequent problem was the fracture of radius at donor site and the limitation of osteotomies in free radius. Similarly, free subscapular flap has been used for restoration of mandibular defects, however the location of the donor site hinders simultaneous harvest of the flap at the time of tumor resection. The use of iliac crest was abandoned due to the short length vascular pedicle and the lack of segmental perforating vessels for osteotomies.4-7
Taylor in 1975 described the free fibula flap, while Hidalgo described its use for mandibular reconstruction.8,9 Since then, the fibula was chosen by various reconstructive surgeons and some of them were able to standardize its use for the restoration of oral cavity defects. Advantages of using fibula as a donor site include available long length of bone and associated soft tissues, near anatomic dimensions, ability to accept bicortical implants and relatively low donor site morbidity.4,8-12 The present study was designed to evaluate the outcome of mandible reconstruction using vascularized free fibula flap, in terms of flap success rate and complications.
This prospective clinical study was carried out at Department of Plastic Surgery, Hayatabad Medical Complex, Peshawar from January 2014 to December 2018. Patients of either gender, who underwent mandibular reconstruction with free fibula oseteocutaneous flap during the study period were included. Diabetic patients with underlying vascular pathologies and cachectic patients were excluded from the study.
The study protocol was approved by the hospital ethical committee. Informed consent was taken from the participants. All the patients were admitted to the hospital. A detailed history of the illness was recorded. Thorough clinical examination and relevant investigations were performed. Prior to the surgical treatment, all the patients were counseled about the procedures along with the associated risks and benefits of the planned surgery.
All the surgeries were performed under general anesthesia and tracheostomies were performed in patients requiring mandibular reconstruction. A hand-held Doppler was used for identification of the perforating vessels supplying the fibula flap. These perforators were marked and the skin paddles were designed to include at least one of the perforating vessels. A tourniquet was applied to the donor lower limb and inflated to create pressure 100 mmHg above the systolic pressure, over the main vessel supplying the lower limb. After cleaning and draping, skin incisions were made over the markings. Retracting the skin and fascia, peroneus longus was retracted anteriorly and the fibula bone was identified. The fibula freed by dissecting from surrounding tissues. The pedicle of the flap was identified, dissected and preserved. The fibula was then harvested with the help of an oscillating saw. At least 6 cm of bone was preserved proximally to prevent injury to peroneal nerve. About 8 cm of distal fibula was left intact for support of ankle. The length of bone needed for reconstruction was measured. Multiple osteotomies were performed for contouring of the bone before dividing the pedicle. After harvesting the free fibula, soft tissues were sutured and skin closure done. Split thickness skin grafts were used where the wound could not be closed primarily. At the end of bone harvest, aseptic dressing of the wound with a posterior splint was applied. The bone was plated and inserted into the defect. The pedicle was positioned along the lingual aspect of the flap. Anastomosis was then performed with standard.
microvascular techniques. At the end of surgery, a nasogastric tube was inserted for feeding.
After the surgery, all patients were started on intravenous antibiotics, analgesics and fluids. Heparin was given for three days and replaced by oral aspirin 75 mg twice daily for 2 weeks. Postoperatively, the flap was clinically monitored. Patients were encouraged to mobilize on the second postoperative day. The donor site dressing was changed on fifth post-operative day and were assessed for graft-take. The wounds were redressed and back slab reapplied. The patients remained hospitalized for 2-3 weeks. Nasogastric feeding was carried out for 3 weeks. Data were analyzed by SPSS version 20. The variables under study were age, sex, operative time, donor site morbidity, flap survival, duration of NG tube feeding and postoperative complications (infection, dehiscence, skin necrosis, delayed wound healing or fistula formation).
There was a total of 56 patients, with 38 (67.85%) males and 18 (32.14%) females. The mean age was 36±10.5 years with an age range of 24-66 years. The mandibular defects resulted from various etiologies: Squamous cell carcinoma (27; 48.21%), giant cell granuloma (3; 5.35%), ameloblastoma, (2; 3.57%), road traffic accidents (10; 17.85%), firearm injury (9; 16%), bomb blast injury (3; 5.35%) and osteoradionecrosis (2; 3.57%). Observed success rate of mandibular reconstruction and associated complications are given in Table I.
Table I: Success rate and complications observed in study participants undergoing mandible reconstruction using vascularized free fibula flap (n=56) |
|
Variables |
Number (%) |
Success rate |
|
Number of flaps survived completely |
52(92.85) |
Complication rate |
|
Wound infections |
13(23.21) |
Skin graft loss at donor site |
5(8.93) |
Complete flap loss |
4(7.14) |
Orocutaneous fistulae |
3(5.36) |
Ankle instability |
2(3.57) |
Skin paddle necrosis |
1(1.78) |
Sensory deficit distal to donor site |
1(1.78) |
Out of the four flaps with complete necrosis, three had venous thrombosis, whereas one had anastomotic disruption due to persistent postoperative hypertension. Patients with partial necrosis of skin paddle were managed with debridement and wound care that resulted in healing with secondary intention. Patients with orocutaneous fistulae were managed with revisional surgery and repair.
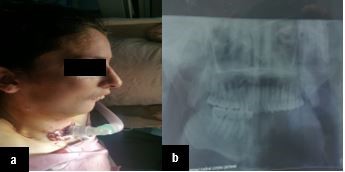 Figure 1: Female patient with post traumatic mandibular defect. (a) Tracheostomy was performed to secure the airway preoperatively. (b) Pre-operative Orthopantomogram (OPG) showing the skeletal defect.
Figure 1: Female patient with post traumatic mandibular defect. (a) Tracheostomy was performed to secure the airway preoperatively. (b) Pre-operative Orthopantomogram (OPG) showing the skeletal defect.
 Figure 2: (a) Post-operative lateral view of the same patient. (b) Post-operative OPG of the same patient.
Figure 2: (a) Post-operative lateral view of the same patient. (b) Post-operative OPG of the same patient.
Defects arising at certain anatomic sites need to be reconstructed with appropriate tissue for a desirable outcome. Mandibular defects are usually difficult to reconstruct primarily due to concerns regarding adequate restoration of function and aesthetics. The main objective in mandibular reconstruction is to repair the bony defects. The aim of management is to restore the stability of bone segment along with appropriate soft tissue coverage.2
Mandible reconstruction is needed in cases of trauma, after tumor resection and necrosis of mandible as complication of radiation therapy to the region.2-4 In the present study, it was observed that oncologic defects of the mandible were the leading cause that required reconstruction. While studying the indications for mandible reconstruction, Sajid et al. and Spzindor also reported this defect as the most common indication,13,14 while Road traffic accidents and firearm injuries are also not uncommon mandibular defects indicating its restoration.15 Certain congenital anomalies, like osteodytstrophy and osteoradionecrosis as a complication of radiation therapy, are also indications for mandible reconstruction.1
The free fibula flap was developed by Taylor and colleagues in 1975.9 Hidalgo described its use for mandibular reconstruction along with the defects of the floor of the mouth in 1989. Three years later he recommended its use for majority of mandibular defects.9,10 Fibula has the advantage of dual blood supply. It has got an endosteal and a periosteal blood supply that makes it a reliable option amongst other flaps. This pattern of blood supply to fibula makes it promising for multiple osteotomies to shape it as mandible.4,11 Another advantage of fibula flap is the availability of long length of the bone. Almost 25 cm of fibula can easily be harvested, which provides sufficient amount of bone to reconstruct a mandible. The flap has an extended length and vessels have a large caliber (artery 2-3 mm and vein 3-4 mm). With large caliber vessels, vascular anastomosis can easily be performed even under the surgical magnifying loupes.4,11-13
The various reconstructive options for mandibular defects include the use of neovascularized bone grafts, titanium reconstructive plates, bone grafts and microsurgical repair with vascularized free osseous and osteocutaneous flaps.1-4 We performed free osteocutaneous flaps for mandible reconstruction along with reconstruction plates in our patients. It was observed that among the 56 flaps performed, only four flaps could not survive yielding a success rate of 91%. This figure can be compared with the results reported by researchers in two separates studies. These studies have reported a success rate of 82.6%, 81.8% and 100% respectively.17,18 Furthermore, they have reported venous thrombosis as a cause of flap failure which is in accordance with our results. Reconstruction of both soft tissues and bone is necessary after the resection of tumors arising from the mandible. Resections may sometimes include adjacent structures like the floor of mouth, tongue and cheek. In addition, a neck dissection in malignant cases may also result in larger defects and even exposure of the vessels. Restoration of all types of tissue with like-tissue has always been challenging and the options for reconstruction are usually not totally satisfactory. Reconstruction of the defects pertaining to the oral cavity along with the mandible are best reconstructed with free fibula osteocutaneous flaps that provide bone and soft tissues simultaneously.4,16-19
Primary reconstruction of the mandibular defects has a major advantage over secondary reconstruction as it is carried out in virgin tissue that are infection free and not manipulated earlier. The tissues are clean and they have no scarring resulting in a reconstructive surgery with optimal functional and esthetic results for the patient. Secondary reconstruction of mandibular defects is usually recommended in cases where there is persistent infection in the previously reconstructed tissue. Execution of surgical procedures in a scarred bed is a tedious task that poses a challenge to the reconstructive surgeon and also badly affect the desirable outcomes.20,21 Primary reconstruction of the mandibular defects is not only cost effective but it also result in early patient mobilization, decreased hospital stay and acceptable functional and aesthetic outcomes.
Vascularized free fibular flap has become the choice of reconstruction for defects of any etiology. This flap is well suitable for the bony defects requiring multiple osteotomies. The additional advantages of free fibula are its anatomic dimension, ability to accept bicortical implants and relatively low donor site morbidity.4,20 Although the large bony defects need to be reconstructed with free flaps, however nonvascularized bone grafts can be used for short bone defects in non-irradiated tissue or in patients not fit to bear the additional operative time required for a free flap reconstruction.17 Patients with advanced tumor usually present with co-morbid conditions and selection of a specific procedure and operating time should be considered to reduce the morbidity and mortality in these selected patients.17 In the present study it took us five and half hours on average to complete the whole procedure of mandible reconstruction with free fibula flap. Other surgeons have also reported almost same time duration for this procedure in their patients.18,21
Microvascular free fibula is a reliable tool for mandibular reconstruction following tumor resection or trauma. The flap has high success rate and fewer complications.
- Kumar BP, Ventakesh V, Kumar KAJ, Yadav BY, Mohan SR. Mandibular Reconstruction: Overview J Maxillofac Oral Surg. 2016; 15(4): 425–41. Doi: 10.1007/s12663-015-0766-5
- Goh BT, Lee S, Tideman H, Stoelinga Paul JW. Mandibular reconstruction in adults: a review. Int J Oral Maxillofac Surg. 2008; 37(7): 597–605. Doi: 10.1016/j.ijom.2008.03.002
- 3. Maurer P, Eckert AW, Kriwalsky MS, Schubert J. Scope and limitations of methods of mandibular reconstruction: a long-term follow-up. Br J Oral Maxillofac Surg. 2010; 48(2): 100–104. doi: 10.1016/j.bjoms.2009.07.005
- Delacure M. reconstruction of the mandible. Indian J Plast Surg. 2007; 40(supplement): 28-34.
- Peled M, El-Naaj IA, Lipin Y, Ardekian L. The use of free fibula flap for functional mandibular reconstruction. J Oral Maxillofac Surg. 2005; 63(2): 220-24. Doi: 10.1016/j.joms.2004.06.052
- Biglioli F, Pedrazzoli M, Autelitano L, Colletti G, Brusati R. The free fibula flap for treating benign mandibular lesions. Minerva Stomatol. 2007; 56(6): 349-58. PMID: 17625492
- Aydin A, Emekli U, Ere M, Hafiz G. Fibula free flap for mandibular reconstruction. Kulak Burun Bogaz Ihtis Derg. 2004; 13(3-4): 62-6. PMID: 16055983
- Taylor GI, Miller GD, Ham FJ. The free vascularized bone graft: a clinical extension of microvascular techniques. Plast Reconstr Surg. 1975; 55(5): 533-44. Doi: 10.1097/00006534-197505000-00002
- Hidalgo DA. Fibula free flap: A new method of mandible reconstruction. Plast Reconstr Surg 1989; 84(1): 71-8. PMID: 2734406
- Hidalgo DA. Aesthetic improvements in free-flap mandible reconstruction. Plast Reconstr Surg 1991; 88(4): 574-85. PMID: 1896529
- Ozalp T, Masquelet AC, Begue TC. Septocutaneous perforators of the peroneal artery relative to the fibula: anatomical basis of the use of pedicled fasciocutaneous flap. Surg Radiol Anat. 2006; 28(1): 54-8. Doi: 10.1007/s00276-005-0059-7
- Shen Y, Guo XH, Sun J, Li J, Shi J, Huang W et al. Double-barrel vascularised fibula graft in mandibular reconstruction: a 10-year experience with an algorithm. J Plast Reconstr Aesthet Surg 2013; 66(3): 364-71. Doi: 10.1016/j.bjps.2012.10.005
- Sajid MAH, Warraich RA, Abid H, Ehsan-ul-Haq M, Shah KL, Khan Z. Reconstruction of mandibular defects with autogenous bone grafts: a review of 30 cases. J Ayub Med Coll Abbottabad. 2011; 23(3): 82-5. PMID: 23272442
- Szpindor E. Evaluation of the usefulness of autogenic bone grafts in reconstruction of the mandible. Ann Acad Med Stetin 1995; 41: 155–69. PMID: 8615541
- MR, Donoff RB. Critical analysis of mandibular reconstruction using AO reconstruction plates. J Oral Maxillofac Surg. 1992; 50(11): 1152–57. Doi: 10.1016/0278-2391(92)90145-p
- Thoma A, Levis C, Young JE. Oromandibular reconstruction after cancer resection. Clin Plastic Surg. 2005; 32(3): 361–375. Doi: 10.1016/j.cps.2005.01.006
- Riaz N, Warraich R. Reconstruction of Mandible by Free Fibular Flap. J Coll Phy Surg Pak. 2010; 20(11): 723-27. Doi: 11.2010/JCPSP.723727.
- Pieptu D, Gogalniceanu D, Getu N, Grosu O, Popescu S, Costan V. Mandibular reconstruction using the free fibula osteocutaneous flap. TMJ. 2005; 55(1): 43-8.
- Nicolic Z, Jeremic J, Milosavjevic R. Use of free microvascular flaps in the management of the head and neck defects. Vojnsanit Pregl. 2006; 63(8): 713-20.
- Rosenthal E, Carroll W, Dobbs M, Wax M, Peters G. Simplifying head and neck micro-vascular reconstruction. Head Neck. 2004; 26(11): 930-36. Doi: 10.1002/hed.20076
- Balaji SM. Total reconstruction of mandible by transport distraction after complete resection for benign and malignanat tumors. Indian J Dent Res. 2016; 27(2): 205-12