Combined Effect of Nicotine and Caffeine on Orthodontic Tooth Movement in Rats
Waseem Akhter1, Erum Yousafzai2, Afia Matloob Rana3, Shakaib Anwar4
1 Associate Professor, Department of Ophthalmology, Rawal Institute of Health Sciences, Islamabad, Pakistan
2 Assistant Professor, Department of Ophthalmology, Rawal Institute of Health Sciences, Islamabad, Pakistan
3 Assistant Professor, Department of Ophthalmology, HBS General Hospital, Islamabad, Pakistan
4 Professor, Department of Ophthalmology, Rawal Institute of Health Sciences, Islamabad, Pakistan
Background:
The individual effects of nicotine and caffeine have been reported in previous studies but their combined effect on tooth movement needs to be elucidated. The objective of this study was to evaluate the combined effect of nicotine and caffeine on the magnitude of orthodontic tooth movement (OTM) in rats.
Material and Methods: This experimental study was conducted on Sprague-Dawley rats (Animal House and Pathology Laboratory; Post Graduate Medical Institute, Lahore) in the department of Orthodontics, de’Montmorency College of Dentistry, Lahore from 8th July 2014 to 8th January 2015. Forty male Sprague-Dawley rats were divided into four equal groups: Control group (CR), nicotine group (NT), caffeine group (CF) and combined nicotine and caffeine group (CNC). Closed coil nickel titanium (NiTi) spring was placed between incisor and maxillary molar. Nicotine group (NT) was treated by intraperitoneal injections of nicotine. Caffeine was given to caffeine group and Combined nicotine and caffeine group (CNC) was treated in the same way as individual nicotine and caffeine groups daily for 14 days. All the rats were sacrificed on 15th day. Magnitude of the orthodontic tooth movement was measured using digital Vernier caliper. Means and standard deviation were calculated for orthodontic tooth movement. One-way ANOVA was used to determine the mean difference in OTM. Post hoc Tukey test was used for multiple comparisons among the groups.
Results:The mean orthodontic tooth movement (OTM) was 0.32 mm ± 0.05 in control group, 0.56 mm ± 0.04 in nicotine group, 0.52 mm ± 0.034 in caffeine group and 0.8 mm ± 0.06 in combined NC group, respectively. The difference between mean OTM among the groups was statistically significant (P-value <0.001). The mean OTM in CNC group was significantly higher as compared to other groups (CR, NT, CF, NT) (P-value <0.001).
Conclusions:In rats, the combined use of nicotine and caffeine results in greater orthodontic tooth movement as compared to their individual use.
Key words: Bone remodeling, Caffeine, Nicotine, Orthodontic tooth movement
The orthodontic tooth movement (OTM) is based on periodontal ligament (PDL) and alveolar bone remodeling which is a complex process depending upon multiple biological mediators, intercellular and cell to matrix interactions1. The applied mechanical force is converted into molecular events that lead to OTM through multifold networked reactions in alveolar bone and PDL cells2. Any change in the biological response may lead to alteration in bone remodeling process and ultimately OTM3.
A number of studies have shown the influence of nicotine on the bone metabolism through its effects on bone remodeling process5. Nicotine stimulated differentiation of osteoclasts in a porcine marrow cell model.5 In a rat study, nicotine increased the bone resorption by induction of interleukin -1, a bone resorbing cytokine6. Similarly a significant increase in the serum levels of bone resorbing cytokines, interleukin-1 (IL-1) and interleukin-6 (IL-6) after administration of nicotine to Sprague-Dawley male rats has also been reported6, 7. Investigations on human gingival fibroblasts have shown that nicotine increases the release of prostaglandin E2 (PGE2) by increasing the expression of cyclooxygenase-2 (COX-2) which influence bone resorption8. On the other hand, it is reported that nicotine decreases the production of type 1 collagen and alkaline phosphatase (ALPase) by osteoblasts and suppresses osteogenesis in cultured human osteosarcoma cells9. The use of nicotine resulted in significant acceleration in the rate of orthodontic tooth movement in rats10.
Similarly, several studies have demonstrated the effect of caffeine on bone metabolism. Caffeine intake is reported to enhance OTM in rats through its effect on alveolar bone remodeling11. Researchers have found association between reduced bone mineral density and caffeine intake in their experiments on rats12. OTM may be enhanced by daily coffee intake through its effect on bone mineral density13. A significant negative relationship between OTM and trabecular bone mass is also demonstrated by Hashimoto et al. in their study on rats14. On the other hand, caffeine is reported to affect the osteoblast function by decreasing 1,25-Dihydroxyvitamin D3 stimulated alkaline phosphatase activity, which is an important marker of osteoblastic activity in human osteoblast cells15.
Caffeine is commonly used psychoactive agent by the children and adults because its use is socially acceptable and it is easily available16. Carbonated and energy drinks, chocolates and coffee are rich sources of caffeine17. Similarly, nicotine is found in many plants as naturally occurring alkaloid. Tobacco and other products like nicotine containing gums are the available sources of nicotine.18 Out of thousands of drugs that are made in the laboratory or found in nature, caffeine and nicotine are among the most widely used legal drugs worldwide19.
The null hypothesis was that combined use of nicotine and caffeine increases the orthodontic tooth movement in a rat model.
This experimental study was conducted on male Sprague-Dawley rats, 10-12 weeks old weighing 200gm (±20) in the department of Orthodontics, de’Montmorency College of Dentistry (DCD), Lahore and Pathology Laboratory, Post Graduate Medical Institute, Lahore from 8th July 2014 to 8th January 2015. All steps described herein conform to the ethical principles for animal research adopted by the US National Institutes of Health and were approved by ethical review committee of DCD and Post Graduate Medical Institute, Lahore (Protocol number 4320/19.9.2019).
The sample size of 40 rats was calculated keeping the power of study at 80% and level of significance to 5%.10 The 40 rats were randomized by lottery method into 4 groups with 10 rats in each group i.e. Control group (CR), Nicotine group (NT), Caffeine group (CF) and Combined Nicotine and Caffeine group (CNC). The rats were housed in the same room and placed in 8 plastic cages (5 per cage), and acclimated to a 12-hour light/dark cycle for 1 week. They had free access to water and standard laboratory rat chow at a temperature of 21°C and humidity of 55%. Nicotine group (NT) was treated by intraperitoneal injections of nicotine, 1mg/1000gm body weight (nicotine tartrate salt, Merck, Darmstadt, Germany, dissolved in normal saline solution).10 Caffeine was given to the caffeine group (CF) as 2.5mg/100gm body weight in drinking water.11 Combined nicotine and caffeine group (CNC) was treated in the same way as individual nicotine and caffeine groups daily for 14 days.
Before placement of an orthodontic appliance, rats were sedated with intramuscular injection of 1.8 mg/kg ketamine and 1.1 mg/kg xylazine, and distance between distal surface of right maxillary first molar and mesial surface of right maxillary second molar was measured. This was followed by ligation of orthodontic appliance between incisor and right maxillary first molar by laceback wire (Morelli, São Paulo, SP, Brazil), using light cure composite adhesive (Transbond XT; 3M/Unitek, Monrovia, Calif) after drilling the tooth surface.10 This appliance comprised of a nickel titanium (NiTi) closed coil spring (Sentaloy®, GAC, NY) delivering a force of 20 cN, measured using a dynamometer tension gauge (MedKraft Orthodontics, USA)6, 10.
All the rats were sedated at 15th day after the placement of appliance with the help of 5.4 mg/kg ketamine to measure the orthodontic tooth movement. This was measured as the distance between distal surface of right maxillary first molar to mesial surface of right maxillary second molar, using calibrated digital Vernier caliper (Fowler High Precision, Newton, Mass). Data was analyzed using SPSS version 20. Means and standard deviation were calculated for orthodontic tooth movement. One-way ANOVA was used to determine the mean difference in OTM. Post-hoc Tukey test was used for multiple comparisons among the groups. A P-value ≤0.05 was considered as statistically significant.
The mean orthodontic tooth movement (OTM) in CR, NT, CF and CNC groups was 0.32 mm ± 0.05, 0.56 mm ± 0.04, 0.52 mm ± 0.034 and 0.8 mm ± 0.06, respectively. One-way ANOVA was applied to compare the mean OTM among groups, which was found to be statistically significant (P-value < 0.001) (Figure 1).
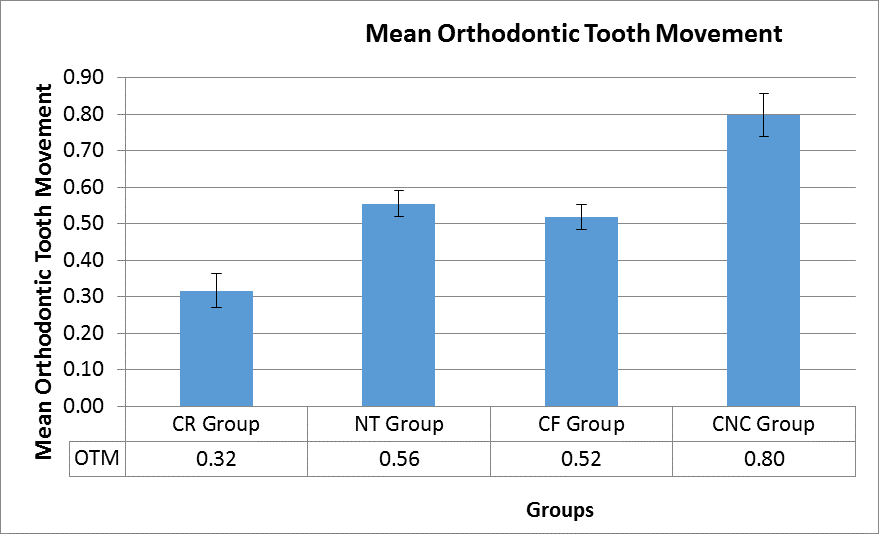
Figure 1: Comparison of mean orthodontic tooth movement among different groups
For multiple comparisons, post hoc Tukey test was used which showed that mean orthodontic tooth movement in CNC group was significantly greater as compared to other groups (CR, NT, CN) (Table I).
When refractive errors were analyzed according to age of patients, it was noted that compound myopic astigmatism was more prevalent in younger ages as compared to older age groups (46.4% vs 19.9%). Mixed astigmatism (18.1% vs 6.3%) and mixed astigmatism combined with presbyopia (38.9% vs 0.7%) were found significantly more common in older ages. Simple myopia was also found significantly greater in younger ages (43.7% vs 15.7%). Overall, the association between different refractive errors and age was statistically significant (P <0.001) (Table III).Table II: Association of refractive errors with gender |
|||
|
Female (n=1294) |
Male (n=844) |
P-value* |
Compound Myopic Astigmatism |
328 (25.3) |
247 (29.3) |
0.07 |
Compound Myopic Astigmatism + Presbyopia |
3 (0.2) |
3(0.4) |
|
Hypermetropia + Presbyopia |
17 (1.3) |
10 (1.2) |
|
Mixed Astigmatism |
160 (12.4) |
75 (8.9) |
|
Mixed Astigmatism + Presbyopia |
95 (7.3) |
83 (9.8) |
|
Presbyopia |
276 (21.3) |
165 (19.5) |
|
Simple Hypermetropia |
37 (2.9) |
30 (3.6) |
|
Simple Hypermetropia + Presbyopia |
18 (1.4) |
12 (1.4) |
|
Simple Myopia |
308 (23.8) |
193 (22.9) |
|
Simple Myopia + Presbyopia |
52 (4.0) |
26 (3.1) |
|
*P-value <0.05 was considered statistically significant
Refractive error is the most common correctable cause of decreased vision in developing countries as well as in Pakistan (43%).14 A survey by Signes-Soler et al in rural Paraguay also listed refractive errors (58%) as the major cause of visual impairment followed by retinal problems.15 According to World Health Organization bulletin 2010 world load of uncorrected refractive errors-related decreased vision (myopia, hypermetropia, astigmatism) is 103 million.14 Different factors effecting the prevalence of refractive errors include selected population (urban or rural), developed or developing country, quality of available eye services, tests and conditions used to evaluate the visual acuity, etc. The current study evaluated the prevalence of different type of refractive errors and their association with different age groups and gender.
Table III: Association of refractive errors with age |
|||||
|
Age categories |
P-value* |
|||
Up to 15 |
16 to 30 (n=412) |
31 to 45 (n=921) |
45 or above (n=453) |
||
Compound Myopic Astigmatism |
113 (32.1) |
191 (46.4) |
183 (19.9) |
88 (19.4) |
<0.001 |
Compound Myopic Astigmatism + Presbyopia |
0 (0.0) |
0 (0.0) |
2 (0.2) |
4 (0.9) |
|
Hypermetropia + Presbyopia |
1 (0.3) |
1 (0.2) |
13 (1.4) |
12 (2.6) |
|
Mixed Astigmatism |
61 (17.3) |
26 (6.3) |
66 (7.2) |
82 (18.1) |
|
Mixed Astigmatism + Presbyopia |
2 (0.6) |
2 (0.5) |
68 (7.4) |
106 (23.4) |
|
Presbyopia |
2 (0.6) |
3 (0.7) |
358 (38.9) |
78 (17.2) |
|
Simple Hypermetropia |
28 (8.0) |
8 (1.9) |
16 (1.7) |
15 (3.3) |
|
Simple Hypermetropia + Presbyopia |
0 (0.0) |
1 (0.2) |
18 (2.0) |
11 (2.4) |
|
Simple Myopia |
145 (41.2) |
180 (43.7) |
145 (15.7) |
31 (6.8) |
|
Simple Myopia + Presbyopia |
0 (0.0) |
0 (0.0) |
52 (5.6) |
26 (5.7) |
|
*P-value <0.05 was considered statistically significant
There was a higher trend of myopia especially myopic astigmatism in our study. Shah et al carried out a population survey on refractive errors in Pakistan and reported myopia (36.5%) as the most common refractive error followed by hypermetropia (27.1%) and astigmatism (37%), respectively16. Similarly a Mexican study by Gomez-Salazar et al. also found myopia as the most common type of refractive error among younger population (10-29 years) and hypermetropia as more common in the older age group17.
In our study the different types of myopia as well as hypermetropia were more common in females (60.5%) as compared to males (39.5%). These results are in accordance with a study carried out by You et al. in Beijing, China18. Other studies on prevalence of refractive errors in Bangladeshi adults by Bourne and colleagues,19 South Indian adult population by Krishnaiah et al20. and a review by Grzybowski et al21. showed that hypermetropic type of refractive error was more common among females. This is in contrast to our study as hypermetropia was more common among our female population. This difference in results can be attributed to factors affecting prevalence mentioned above, like urban vs rural, developed vs
developing country or availability of eye services, etc.
Compound myopic astigmatism was more prevalent in younger ages as compared to older age groups (46.4% vs 19.9%). Mixed astigmatism (18.1% vs 6.3%) and mixed astigmatism combined with presbyopia (38.9% vs 0.7%) were found significantly more common in older ages. Simple Myopia was also found significantly greater in younger ages as compared to older age groups (43.7% vs 15.7%). Younger age myopia was also more prevalent (52.2%) in a study done by Yingyan et al22.
The uneven distribution of trained health services and institution among rural and urban population is a major challenge making it difficult for patients with refractive errors to approach these services23, 24. World Health Organization in the global action plan of 2014-2019 for "Universal eye health” also identified provision of resources and development of national policies for prevention of avoidable visual impairment, specifically refractive errors25.
The major strength of this study was a large sample size and use of both objective and subjective refraction for testing of visual acuity. The main limitation of the study was that patients with refractive errors were enrolled from one institution only; therefore, findings cannot be generalized to the whole rural population of Islamabad.
The prevalence of myopia and hypermetropia is significantly higher among female population and younger individuals of rural area of Islamabad while mixed astigmatism combined with presbyopic type of refractive error is more common among elderly population.
- Rensikoff S, Pascolini D, mariotti SP, Pokharel GP. Global magnitude of visual impairment caused by uncorrected refractive errors in 2004. Bull World Health Organ. 2008; 86(1):63-70. Doi: 10.2471/blt .07.041210
- Solange RS, Rafael WC, Adriana B, Luana M, Célia R. Nakanami, et al. Prevalence and causes of visual impairment in low–middle income school children in São Paulo, Brazil. Invest Ophthalmol Vis Sci. 2008; 49(10): 4308–13. Doi: 10.1167/iovs.08-2073
- Pirro GH, Omar AM, Phillippa C, Robert W, Katie MW, Terri LY, et al. Common mechanisms underlying refractive error identified in functional analysis of gene lists from genome-wide association study results in 2 european british cohorts. JAMA Ophthalmol. 2014; 132(1): 50–6. Doi: 10.1001/ jamaophthalmol.2013.6022
- John C, Chiu-Fang C, Matthew MZ, Xinzhi Z, Kai MB, Alan RM, et al. The association of health-related quality of life with severity of visual impairment among people aged 40–64 years: findings from the 2006–2010 behavioral risk factor surveillance system. Ophthalmic Epidemiol. 2016; 23(3): 145-53. Doi: 10.3109/09286586.2016.1168851
- Van CL, Kristen AE. VISION 2020: The right to sight in 7 Years? Med Hypothesis Discov Innov Ophthalmol. 2013; 2(2): 26–9. PMID: 24600638
- Pizzarello L, Abiose A, Ffytche T, Duerksen R, Thulasiraj R, Taylor H, et al. VISION 2020: The right to sight. a global initiative to eliminate avoidable blindness. Arch Ophthalmol. 2004; 122(4): 615–20. Doi: 10.1001/archopht.122.4.615
- Siegwart JT, Norton TT. Perspective: How might emmetropization and genetic factors produce myopia in normal eyes? Optom Vis Sci. 2011; 88(3): 365–72. Doi: 10.1097/OPX.0b013e31820b053d
- Rafael I, Hassan H, Mehdi K, Ian GM, Emamian MH, Shariati M, et al. Hyperopia and lens power in an adult population: the shahroud eye study. J Ophthalmic Vis Res. 2015; 10(4): 400–07. Doi: 10.4103/2008-322X.158895/li>
- Flitcroft DI. Emmetropisation and the aetiology of refractive errors. Eye (Lond). 2014; 28(2): 169–79. Doi: 10.1038/eye.2013.276
- Stambolian D. Genetic susceptibility and mechanisms for refractive error. Clin Genet. 2013; 84(2): 102–8. Doi: 10.1111/cge.12180
- AK SM, Pourmazar R, Gohary, I. Awareness and attitude toward refractive error correction methods: a population-based study in mashhad. Patient Saf Qual Improv. 2013: 1(1):23-9.
- Suraj SS, Praveen VN, Sumit M, Vasundhara M, Bhardwaj A, Vivek G. Prevalence of visual impairment due to uncorrected refractive error: Results from Delhi-Rapid Assessment of Visual Impairment Study. Indian J Ophthalmol. 2016; 64(5): 387–90. Doi: 10.4103/0301-4738.185614
- Islamabad Capital Territory Administration. Archived 4th April 2011 at the Wayback Machine. Ictadministration.gov.pk. Retrieved on 14 June 2020. http://www.ictadministration.gov.pk/
- Pascolini D, Mariotti SP. Global estimates of visual impairment: 2010. Br J Ophthalmol. 2012; 96(5): 614–18. Doi: 10.1136/bjophthalmol-2011-300539
- Signes-Soler I, Hernández-Verdejo JL, Lumeras MA, Verduras ET, Piñero DP. Refractive error study in young subjects: results from a rural area in Paraguay. Int J Ophthalmol. 2017; 10(3): 467–72. Doi: 10.18240/ijo.2017.03.22
- Shah SP, Jadoon MZ, Dineen B, Bourne RR, Johnson GJ, Gilbert CE, et al. Refractive errors in the adult Pakistani population: the national blindness and visual impairment survey. Ophthalmic Epidemiol. 2008; 15(3): 183-90. Doi: 10.1080/0928658080 2105822
- Gomez-Salazar F, Campos-Romero A, Gomez-Campaña H, Cruz-Zamudio C, Chaidez-Felix M, Leon-Sicairos N, et al. Refractive errors among children, adolescents and adults attending eye clinics in Mexico. Int J Ophthalmol. 2017; 10(5): 796–802. Doi: 10.18240/ijo.2017.05.23
- You QS, Wu LJ, Duan JL, Luo YX, Liu LJ, Li X, et al. Prevalence of myopia in school children in greater Beijing: the Beijing Childhood Eye Study. Acta Ophthalmol. 2014; 92(5): 398–406. Doi: 10.1111/ aos.12299
- Bourne RR, Dineen BP, Ali SM, Huq DM, Johnson GJ. Prevalence of refractive error in Bangladeshi adults: results of the National Blindness and Low Vision Survey of Bangladesh. Ophthalmol. 2004; 111(6): 1150-60. Doi: 10.1016/j.ophtha.2003.09.046
- Krishnaiah S, Srinivas M, Khanna RC, Rao GN. Prevalence and risk factors for refractive errors in the South Indian adult population: The Andhra Pradesh Eye disease study. Clin Ophthalmol. 2009; 3:17-27. PMID: 19668540
- Grzybowski A, Kanclerz P, Tsubota K, Lanca C, Saw SM. A review on the epidemiology of myopia in school children worldwide. BMC Ophthalmol. 2020; 20(1): 27. Doi:10.1186/s12886-019-1220-0
- Ma Y, Qu X, Zhu X, Xu X, Zhu J, Sankaridurg P, et al. Age-specific prevalence of visual impairment and refractive error in children aged 3–10 years in Shanghai, China. IOVS. 2016; 57(14): 6188-96. Doi: 10.1167/iovs.16-20243
- Gilbert CE, Shah SP, Jadoon MZ, Bourne R, Dineen B, Khan MA, et al. Poverty and blindness in Pakistan: results from the Pakistan national blindness and visual impairment survey. BMJ. 2008; 336(7634): 29–32.
- Wang W, Yan W, Müller A, Keel S, He M. Association of Socioeconomics with Prevalence of Visual Impairment and Blindness. JAMA Ophthalmol. 2017; 135(12): 1295–1302.
- Gupta N, Kocur I. Chronic eye disease and the WHO Universal Eye Health Global Action Plan 2014-2019. Can J Ophthalmol. 2014; 49: 403–4