Marsupialization Followed by Enucleation and Chemical Cauterization for Treatment of Odontogenic Keratocyst Involving Maxillary Sinus: A Case Report
Muhammad Jamal1, Muhammad Zeeshan Baig1, Laiba Saher2, Muhammad Asim2
1 Assistant Professor, Department of Oral and Maxillofacial Surgery, Islamabad Medical and Dental College Islamabad
2 Postgraduate Resident, Department of Oral and Maxillofacial Surgery, Islamabad Medical and Dental College, Islamabad
Odontogenic keratocysts are odontogenic cysts which have locally infiltrative behavior. They mostly occur in second and fourth decades but can occur at any age throughout life. In majority of cases, they are located in the posterior region of mandible, but can also be found in the maxilla especially in the canine region. In this article, we have discussed the diagnosis and management of a large odontogenic keratocyst cyst involving the maxillary sinus. A 22 years old male patient presented with pain and swelling on right side of the face since last one year. There was history of pus discharge and gradual increase in size of the swelling since last 3-4 months. Patient took antibiotics but there was no improvement. Odontogenic keratocyst is a developmental pathology which arises from additional remnants of dental lamina of oral epithelium. They present with swelling, pain and pus formation/discharge as signs of infection. Often, when the lesion is large there can be paresthesia of the lower lip. These lesions can also be clinically asymptomatic. Mostly they appear as well-demarcated unilocular radiolucency having a thin, sclerotic well-defined margin. There are many treatment options like enucleation, marsupialization, decompression, curettage, use of chemical agents like Carnoy's solution, cryotherapy with liquid nitrogen or peripheral osteotomy and surgical resection of lesion.
Key Words: Chemical cauterization, Enucleation, Marsupialization, Maxillary sinus, Odontogenic kerotocyst
Odontogenic keratocysts (OKC) are odontogenic cysts which have locally infiltrative behavior.1 Odontogenic keratocysts mostly occur in second and fourth decades but can occur at any age throughout life. They have a predilection for males and are more frequent in the posterior region of the mandible.2 Most of the cases are incidentally discovered on routine radiographs for dental problems. Mostly they appear as well-demarcated unilocular radiolucency having a thin, sclerotic well-defined margin. They can be multilocular or unilocular in nature, frequently penetrating the cortical bone of the jaw and adjacent anatomical structures. Many times, teeth which are in approximation can be displaced and no root resorption occurs.1Involvement of the maxillary sinus by OKC is rare with <1% of cases reported in the literature.3 The maxillary sinus is a part of the paranasal sinuses, in proximity with developing tooth and root apices of premolar and molars. It is vulnerable to odontogenic infection, cyst and tumors of odontogenic origin. Diagnosis of such lesion is challenging as maxillary radiographs do not offer characteristic features due to overlapping of various structures.2
A 22-year-old male patient presented to OMFS department with the complaints of pain and swelling on the right side of face for last one year. Since last 3-4 months, there was gradual increase in size of the lesion. There was a history of pus discharge intraorally from upper right posterior teeth since last few months. Patient was taking antibiotics for pain and swelling since last 3 months. Clinically there was diffuse firm swelling involving the right maxillary premolar-molar region. Permanent canine was missing in the arch and the deciduous canine was present intraorally. Upper right premolars and first molar teeth were non-vital. Patient was advised OPG which showed impacted canine and radiolucency involving the premolar and first molar. Biopsy was done and specimen was sent for histopathology examination. The lesion was diagnosed as odontogenic keratocyst. Patient was sent for CT Scan, which showed well defined lobulated cystic lesion arising from right maxillary alveolus and extending into the ipsilateral maxillary sinus superiorly (Figure 1a). The lesion was centered around the crown of impacted right maxillary canine tooth measuring 3.8x2.2x3cm. There was bony erosion of the lateral wall of the lesion adjacent to the mesial border of the masseter muscle and anterior border of lateral pterygoid (Figure 1b). Posteriorly, it was limited by the posterior wall of the maxillary sinus and body of pterygoid bone and its plates were well-preserved. Patient was informed about the clinical condition and with his consensus, marsupialization was planned.
Under local anesthesia, right upper vestibular incision was made in premolar-molar region. The lesion was exposed (Figure 2a), irrigated and nasopharyngeal airway tube (cut to fit the size of the lesion) was placed and sutured with the surrounding mucosa. Patient was given Tablet Augmentin (625mg), Tablet Gramex (400mg) and Tablet Torex IR (550mg) for 5 days and advised daily irrigation, maintenance of good oral hygiene and regular follow up. Also, the involved teeth were endodontically treated. Follow up radiograph (OPG) was advised after 3 months. On follow up visit following surgery, size of the lesion and white cheesy discharge was reduced and there was no pus discharge. CT scan was advised 6 months post-marsupialization, which showed regression in size of the lesion (now measuring 1.8 x 2.3 x 1.9 cm), thick and smooth walls with internal foci of calcification along internal wall. Bony erosion of the lateral wall of the lesion was still present. As the lesion was responding to marsupialization, it was planned to continue the same treatment for another 6 months. However, the patient was not willing to continue with a prolonged treatment, so enucleation with chemical cauterization under general anesthesia (GA) was planned as an alternative.
All the pre-operative work up for GA fitness was done and surgery planned. Under aseptic measures, standard draping and GA, nasopharyngeal airway tube placed for marsupialization was removed and right upper vestibular incision made from canine to second molar region. Flap was elevated and the lesion was exposed.
The lining of the lesion was detached from maxillary sinus membrane and overlying mucosa without disrupting the continuity of sinus membrane (Figure 2b, c & d). Impacted canine was exposed, sectioned and removed along with the lining (Figure 2e, f & g). Apicectomy of the involved endo-treated teeth was performed. Gauze soaked in Corney`s solution was placed in the cavity for 3 minutes after which the cavity was irrigated with copious saline, hemostasis achieved and the incision was closed with 3-0 vicryl. Intraoral tail pack was placed in the oral cavity and the patient was shifted to the ward in a stable condition after recovery. Patient was on regular follow up with post-operative radiograph at 3-month, 6 month and 1-year interval (Figure 3) to rule out recurrence and amount of bone formation during healing.
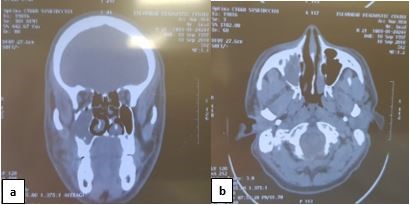 Figure 1: (a) Coronal view shows the lesion involving the entire right maxillary sinus. (b) Axial view shows the lesion causing bony erosion of the lateral wall of maxillary sinus
Figure 1: (a) Coronal view shows the lesion involving the entire right maxillary sinus. (b) Axial view shows the lesion causing bony erosion of the lateral wall of maxillary sinus
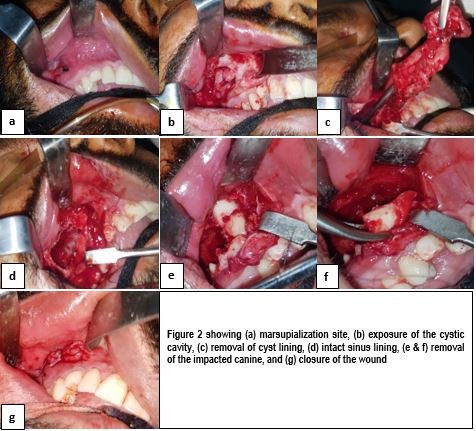
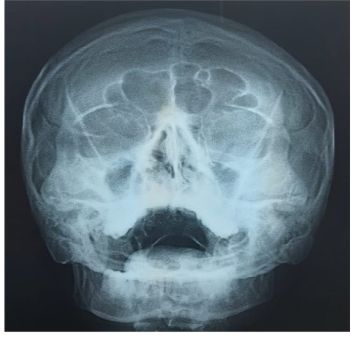 Figure 3: Post-operativeoccipitomental view one year after surgery showing normal maxillary sinus with no haziness and adequate distal bone formation
Figure 3: Post-operativeoccipitomental view one year after surgery showing normal maxillary sinus with no haziness and adequate distal bone formation
Odontogenic keratocyst is a developmental pathology which arises from additional remnants of dental lamina of oral epithelium. It is 2-11% of all odontogenic cysts, can occur at any age throughout life and has a male to female ratio of 2:1.4 OKC involves both the jaws, but the mandible is more often involved than the maxilla.
In mandible, the highest frequency occurs in the body of the mandible (20%) followed by the angle of the mandible (18%) and vertical ramus (10%), but in the maxilla, it is seen most commonly in the canine area, followed by third molar tuberosity and anterior maxilla.2,3 Maxillary sinus pathology can occur when the Schneiderian membrane is breached by conditions such as the odontogenic pathology of the maxillary bone. Odontogenic infections and pathology account for 11%–12% cases of maxillary sinusitis.3
OKCs presents with swelling, pain and pus formation/discharge as signs of infection. Often, when the lesion is large, there can be paresthesia of the lower lip. These lesions can also be clinically asymptomatic. They are often associated with basal cell naevus syndrome, also called as Gorlin's syndrome, in which there are OKC lesions, skin basal cell carcinomas, falx calcifications and skeletal abnormalities. A perceptible number of cases are diagnosed incidentally during regular dental inspections.4,5
Radiographs show unilocular or multilocular radiolucency with uniform sclerotic borders which may be involving an unerupted tooth, mostly impacted third molar. Bone expansion is not well noted.6 On histopathological examination, a cystic lining with desquamated epithelium, 6-10 cell thick lining of para keratinized stratified squamous epithelium with palisading basal cell layer of even thickness is seen.7
There are many treatment options like enucleation, marsupialization, decompression, curettage, use of chemical agents like Carnoy's solution, cryotherapy with liquid nitrogen or peripheral osteotomy and surgical resection of lesion.5,8 The choice of treatment is decided on various factors which include age, size and recurrence. But generally, in young patients, conservative treatment is always preferred.5 Marsupialization has a promising outcome. In large lesions, if surgical approach is selected, there are chances of damage to adjacent structures like maxillary antrum and inferior alveolar canal. When treating large lesions, enucleation should be done to avoid sinusitis, mandibular fracture, mandibular continuity defect or fistulae formation of any form. Allon and colleagues have quoted a number of studies advocating the use of decompression plus marsupialization as a definitive treatment approach.9
Chemical cauterization is a treatment choice for the keratocystic odontogenic tumor. Previously, Carnoy’s solution composing of ethanol, chloroform, glacial acetic acid, ferric chloride was used because of its hemostatic action and local fixation. However, FDA restricted agents that contained chloroform and since then Carnoy’s solution is made without chloroform.9 Because of increased mitotic activity, OKC has increased aggressiveness. The epithelial cells of OKC and microcysts, are often found in the mucosa of the alveolar ridges which can cause recurrence.10,11 Long term follow-up with clinical and radiographic examination is essential up to five post-surgical years to rule out recurrence.12
Accurate diagnosis of odontogenic keratocysts is essential for proper therapy and follow-up. Marsupialization results in new bone formation and thickening of the cyst wall and makes enucleation at a later stage easier. Treatment of odontogenic keratocysts by enucleation and chemical cauterization using carnoy’s solution shows a low recurrence rate. Adherence to a therapeutic protocol in the treatment of OKC and systematic and long-term postoperative follow-up are key elements of a successful outcome.
- Santos RS, de Moraes Ramos-Perez FM, do Amaral Silva GK, Rocha AC, Prado JD, da Cruz Perez DE. Odontogenic keratocyst: the role of the orthodontist in the diagnosis of initial lesions. Am J Orthod Dentofacial Orthop. 2017; 152(4): 553-6. Doi: 0.1016/j.ajodo.2017.06.013
- Mortazavi H, Baharvand M, Safi Y, Behnaz M. Common conditions associated with displacement of the inferior alveolar nerve canal: A radiographic diagnostic aid. Imaging Sci Dent. 2019; 49(2): 79-86. Doi:10.5624/isd.2019.49.2.79
- Sheethal HS, Rao K, Umadevi HS, Chuhan k. Odontogenic keratocyst arising in the maxillary sinus: A rare case report. J oral Maxfac Pathol. 2019; 23 (Suppl 1): 74-7. Doi: 10.4103/jomfp.JOMFP_319_18
- Marcelis S, Van Damme S, Vanhoenacker F. Odontogenic keratocyst of the mandible. Eurorad. 2018. Doi: 10.1594/EURORAD/CASE.16132
- de Molon RS, Verzola MH, Pires LC, Mascarenhas VI, da Silva RB, Cirelli JA, Barbeiro RH. Five years follow-up of a keratocyst odontogenic tumor treated by marsupialization and enucleation: a case report and literature review. Contemp Clin Dent. 2015; 6 (Suppl 1): S106. Doi: 10.4103/0976-237X.152963
- de Castro MS, Caixeta CA, de Carli ML, Júnior NV, Miyazawa M, Pereira AA, Sperandio FF, Hanemann JA. Conservative surgical treatments for nonsyndromic odontogenic keratocysts: a systematic review and meta-analysis. Clin Oral Investig. 2018; 22: 2089-101.
- Tarallo AM, de Souza Matos F, de Souza VF, Paranhos LR, Herval ÁM, Valera MC, Carvalho CA. Odontogenic Keratocyst: A Case Report Emphasizing on Root Canal Treatment after Surgical Intervention. IEJ. 2019; 14(2):160-5. Doi: 10.22037/iej.v14i2.23984
- Ecker J, ter Horst R, Koslovsky D. Current role of carnoy's solution in treating keratocystic odontogenic tumors. J Oral Maxillofac Surg. 2016; 74(2): 278-82. Doi: 10.1016/j.joms.2015.07.018
- Allon DM, Allon I, Anavi Y, Kaplan I, Chaushu G. Decompression as a treatment of odontogenic cystic lesions in children. J Oral Maxillofac Surg. 2015; 73(4): 649-54. Doi: 10.1016/j.joms.2014.10.024
- US Food and Drug Administration. "Sec. 460.200 in FDA compliance policy guides." FDA, Washington, DC: 219, 1992.
- Slusarenko da Silva Y, Naclério-Homem MG. Conservative Treatment of Primary and Nonsyndromic Odontogenic Keratocyst: An Overview of the Practice. Int J Oral Dent Health. 2018; 4: 070. Doi: 10.23937/2469-5734/1510070.
- Gnanaselvi UP, Kamatchi D, Sekar K, Narayanan BS. Odontogenic keratocyst in anterior Mandible: An interesting case report. J Indian Acad Dent Spec Res. 2016; 3: 22. Doi: 10.4103/2229-3019.192466.