Patterns of Developmental Delay in Children with Autism Spectrum Disorder: A Perspective from a Developing Country
Rehmana Waris1 ,Hashim Raza2 ,Ramish Riaz3
1Children's Hospital, Pakistan Institute of Medical Sciences, Islamabad, Pakistan.
2Department of Medical Imaging Technology, FRAHS, Riphah International University, Islamabad, Pakistan
Background:: Autism Spectrum Disorder is a developmental disorder characterized by
difficulties in social interaction, initiating conversations, delay in language skills, play
skills, and stereotypic behaviours. Children with severe developmental delays and those with
global developmental delays need to be identified as they may have long-term problems and
disabilities.
Objective: To compare the conservative management with active management of
prelabor premature rupture of membranes at 34–37 weeks of gestation.
Material & Methods:All children below the age of 5 years coming first time for
assessment of ASD and diagnosed using ADI-R and ADOS-2 were included in the study. A total of
334 children met the criterion. All children having performance deficits below 2SD on
age-appropriate mean were considered as having developmental delays. Those having delays in two
or more domains were labelled as having global developmental delays. Detailed clinical and
developmental assessment was performed. Data was entered and analyzed via SPSS v26.
Results:: Out oMean age of children at the time of presentation was 3.6±1.10 years
with male to female ratio of 3.5:1. According to developmental assessment using Schedule for
growing Scales II, the most affected area was speech and language (51.5%) followed by cognitive
skills (50.7%), social interactive skills (49.9%), visual skills (46.9%), hearing and language
skills, (38.3%), self-care social skills (26.2%), manipulative skills (13.5%) and gross motor
skills (0.4%). Global Developmental Delay was found to be present in half of the children for
which there was no other possible explanation.
Conclusion:: Most of the children with Autism Spectrum Disorder had developmental
delays of some sort. Therefore, every child with Autism Spectrum Disorder must be evaluated for
Developmental Delay and supported.
Key words:Autism Spectrum Disorder, Developmental Milestones, Global Developmental
Delay, Speech Delay, Social Skills, Cognitive delay
Autism Spectrum Disorder is a developmental disorder characterized by difficulties in social
interaction, initiating conversations, delay in language skills, play skills, and stereotypic
behaviours including repetition, hypersensitivity or hyposensitivity to sensory experiences.
Some may show hyperactivity and aggression.1Children and individuals with Autism
Spectrum
Disorder also face difficulties in regulating emotions and have decreased EQ (emotional
quotient).2Fifty percent of these individuals show intellectual disabilities and have
lower IQ
(Intellectual Quotient) levels than their peers.3Till now aetiology of autism is
poorly
understood. Both environmental and genetic factors are thought to play a role in its
development. Other causative factors are also thought to play a role though evidence is not
established yet. Co-morbidities that can occur with Autism include seizures, immune disorders,
Attention Deficit Hyperactivity Disorder, obsessive-compulsive disorder, Learning Disabilities,
Dyslexia, and other behavioral disorders.4
According to WHO, 1 in 160 children has Autism Spectrum Disorder.5In America,
according to the
latest study, 1 in 36 children are affected.6In Pakistan, the prevalence of ASD is
not known
due to a lack of awareness. Though 19 in 1000 children have learning disabilities and 16 in 1000
have severe mental retardation. Due to lack of knowledge and trained professionals for
developmental disorders, most of the children are misdiagnosed. Most of the general public
consider it as mental illness and there is a huge social stigma attached to such diseases.
Subsequently, parents of such children avoid contact with healthcare professionals or seek
medical attention very late. However, in the urban population, the trend is
changing.7Autism
generally come into notice at pre-school when a child is unable to cope socially with other
children although specific criterion has been developed to diagnose it at an early age. The
absence of babbling, and lack of social smile till 1 year is one of the prominent signs of ASD
that must alert parents.8
Many scales have been developed to diagnose ASD. However most commonly used tool for its
diagnosis is the Autism Diagnosis Observation Schedule (ADOS).9It is a standardized
semi-structured evaluation of social interaction, imaginative play, communication skills, and
behaviors. ADOS-2 was released in 2012, has five modules, and is currently considered as gold
standard, Toddler Module is for children from 13 to 30 months without speech, Module 1 is for
children aged 31 months and those older without speech, Module 2 is for children with speech but
not fluent, Module 3 for children and adolescents with fluent speech, Module 4 for adults with
fluent speech.10
Children with ASD have different developmental courses than other children. They have delays in
some domains but achieve some milestones earlier. However, it is different from general
developmental delay and should be differentiated from it as both require different management
though both conditions may co-exist. Developmental delay typically implies to delay in the
achievement of developmental milestones and can be graded into mild, moderate, and severe.
Global developmental delay refers to intellectual delays with impairment in two or more adaptive
skills.11Children with developmental delays have the risk of lifelong intellectual
and physical
disabilities. Early diagnosis and intervention can improve the outcome and help children achieve
their potential. Studies have shown that children with Autism have experienced mild
developmental delays in motor and language skills and deficits in social skills. However, these
delays are more common in children below 3 years and gradually improve with age.12It
is also
reported that 30 to 60 percent of children with ASD also suffer from intellectual
disability.13
Developmental delays are usually diagnosed via detailed clinical and developmental assessment to
check developmental status in all domains i.e. locomotor skills, manipulative skills, visual
skills, hearing and language skills, speech and language skills, social interactive skills,
self-care social skills and cognitive skills.14Schedule for Growing Skills 11(SGS II)
is one of
the scales to assess developmental status in children less than 6 years old.15Other
investigations are usually carried out to diagnose the underlying genetic or structural
pathologies.16
For treating Autism different interventional strategies related to individual symptoms improve
the condition and ability to participate in society. Most of the strategies include occupational
therapy, speech therapy, and social skills training. No medications are usually prescribed for
core symptoms of ASD children however when patients have co-morbidities like seizure,
behavioural issues, suicidal thoughts, or other conditions medications are
considered.17The
current study focuses on the presence of developmental delay and its patterns in children
affected with ASD in Pakistan.
This descriptive study was conducted at Children's Hospital, Pakistan Institute of Medical Sciences from May 2017 to April 2020. All children ≤5 years coming first time for assessment of ASD and diagnosed with it on ADI-R and ADOS-2 were included in the study. A total of 334 children met the criterion. All children having performance deficits below 2SD on age-appropriate mean in motor skills, manipulative skills, visual skills, speech and language skills, hearing and language skills, social interaction skills, self-care social skills, and cognitive skills were considered as having developmental delay classified by using SGS-II. Those having delays in two or more domains were labeled as having global developmental delays. A detailed clinical assessment was performed, and past medical and family history was taken. Family history was considered positive if any of the relatives had any kind of developmental delay not necessarily ASD. Data were entered and analyzed in SPSS v26. Descriptive statistics were performed on qualitative data, dispersion in data was analyzed via mean and standard deviation measurement, relative risk, and Odd’s Ratio was applied for risk assessment. .
The mean age of children at the time of presentation was 3.6±1.10 years. The majority (n=259,
77.5%) of the patients were males with a male-to-female ratio of 3.5:1. Twenty-six percent
(n=89) of the cases had positive family history (Figure-1).
A most common complaint was speech delay followed by repetitive behaviour, behavioural issues,
poor social interaction, non-responsiveness, lack of imaginative play and sensory issues
(Figure-2). The mean age of neck holding was 3.87 ± 2.0months, starting sitting was 7.9 ± 2.56
months, crawling was 10.88 ± 4.3 months, walking was 15.6 ± 6.1 months, social smile was 3.71 ±
2.9 months, vocalization was 8.43 ± 7.6 months and babbling was 10.68 ± 3.55 months. The
majority of the children had both weight (79%) and OFC (94%) below 25th percentile. Few children
(n=29, 8.68%) presented with co-morbidities. Most common were epileptic seizures (n=14) followed
by ADHD (n=6), Deafness (n=3), Down’s Syndrome (n=1), Tuberous Sclerosis (n=1), Factor 5
deficiency (n=1), Microcephaly (n=1), Albinism (n=1) and Hypothyroidism (n=1).
According to the SGS-II scale most affected area was speech and language (51.5%) followed by,
cognitive skills (50.7%), social interactive skills (49.9%), visual skills (46.9%), hearing and
language skills, (38.3%), self-care social skills (26.2%), manipulative skills (13.5%) and gross
motor skills (0.4%) (Figure-3).
Detailed analysis showed females to have more delay in all domains i.e. gross motor skills
(1.62%), manipulative skills (16.13%), visual skills (51.6%), speech and language (62.91%),
hearing and language (50%), interactive social skills (56.46%) cognitive skills (61.2%) and
self-care social skills (20.97%) compared to male with gross-motor skills (0%), manipulative
skills (6.04%), visual skills (45.46%), speech and language (48.2%), hearing and language
(36.8%), interactive social skills (48.2%), cognitive skills (48.6%) and self-care social skills
(11.4%) (Figure-4). A significant difference was found between the female gender and specific
skills (Table 1).
Toddlers had more delay in visual skills (57.04%), hearing and language skills (38.92), speech
and language skills (54.36%), cognitive skills (55.03%) compared to pre-schoolers with
manipulative skills (12.03%), visual skills (44.36%), hearing and language skills (37.59),
speech and language skills (48.12%), cognitive skills (44.36%). Pre-schoolers had more delay in
manipulative skills (12.03%) and gross motor skills (0.75%) compared to toddlers with
manipulative skills (6.09%) and gross motor skills (0%). However, no significant difference was
found between both age groups, and specific skills (Table-2).
Global Developmental Delay was found to be present in half (n=167, 50.0%) of the children.
Toddlers had more GDD than pre-schoolers (Figure 4). Among factors studied for the risk of
global developmental delay only the presence of co-morbid conditions was found to be associated.
Relative risk of GDD was found to be significantly increased if child presented with sensory
symptoms and non-responsiveness (Table-3).
GDD was found to be more common in toddlers in comparison to pre-schoolers. Gender was found to
be independent of GDD (Figure 4).
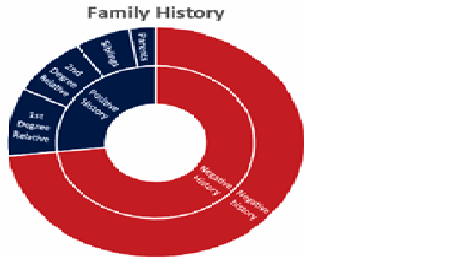
Figure-1: Family History of the Children with Autism Spectrum Disorder
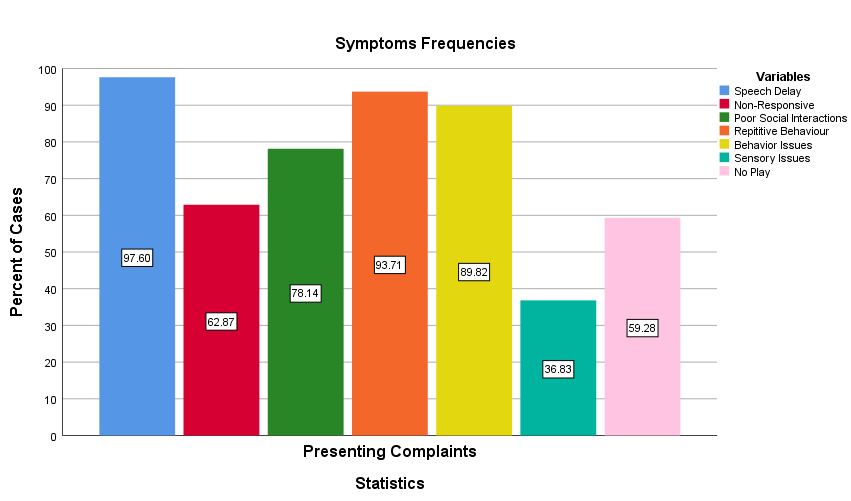
Figure 2: Presenting complaints of the children with Autism Spectrum Disorder
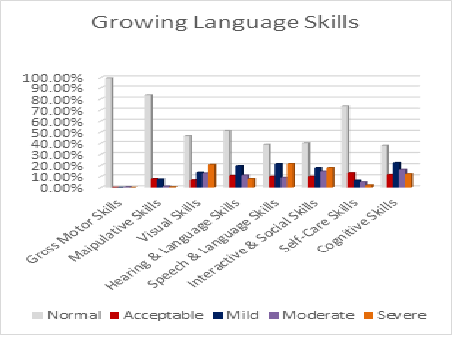
Figure 3: SGS score of the children with Autism Spectrum Disorder
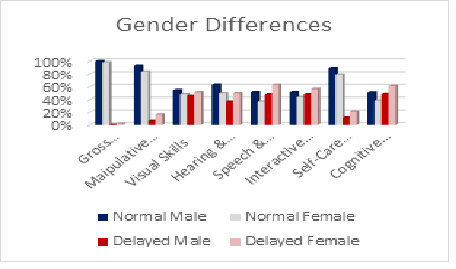
Figure-4- Gender differences and Developmental Delays in Autistic Children
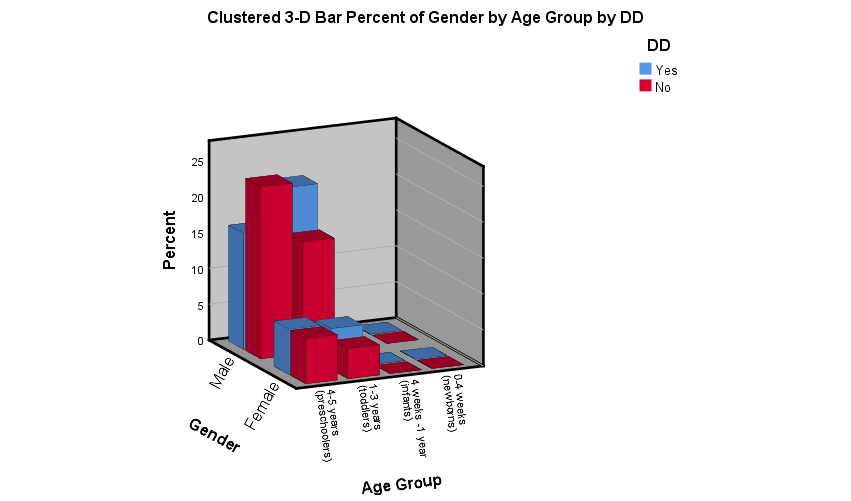
Figure-5: Age versus Gender wise distribution of Global Developmental Delay in Children with Autism Spectrum Disorder
|
Table-1 Gender Wise Developmental Assessment Taking Females as Exposed Group |
|||
|
|
Odd’s Ratio |
Relative Risk |
P-Value |
|
Gross Motor Skills |
10.7 |
10.2 |
0.14 |
|
Manipulative Skills |
2.75 |
2.36 |
0.001 |
|
Visual Skills |
1.28 |
1.18 |
0.3 |
|
Hearing Skills |
1.48 |
1.3 |
0.1 |
|
Speech Skills |
1.5 |
1.2 |
0.2 |
|
Social Skills |
1.91 |
1.8 |
0.002 |
|
Self-Care Skills |
2.06 |
1.7 |
0.005 |
|
Cognitive Skills |
1.69 |
1.22 |
0.007 |
|
Table-2: Age Group Wise Developmental Assessment taking Toddler as Exposed Group |
|||
|
|
Odd’s Ratio |
Relative Risk |
P-Value |
|
Gross Motor Skills |
0.2 |
0.1 |
0.4 |
|
Manipulative Skills |
0.5 |
0.4 |
0.08 |
|
Visual Skills |
2.54 |
1.66 |
0.001 |
|
Hearing Skills |
1.04 |
1.06 |
0.8 |
|
Speech Skills |
1.54 |
1.24 |
0.07 |
|
Social Skills |
0.8 |
0.7 |
0.2 |
|
Self-Care Skills |
0.8 |
0.7 |
0.2 |
|
Cognitive Skills |
1.5 |
1.24 |
0.07 |
|
Table-3: Factors affecting Risk of Global Developmental Delay in Autistic Children |
|||
|
|
Odd’s Ratio |
Relative Risk |
P-Value |
|
Factors |
|
|
|
|
Co-Morbid |
1.88 |
1.35 |
0.05 |
|
Family History |
1.2 |
1.1 |
0.63 |
|
Weight above the 75 th percentile |
0.8 |
0.7 |
0.2 |
|
OFC at birth below the 25 th percentile |
0.86 |
0.7 |
0.2 |
|
Female Gender |
1.14 |
1.08 |
0.5 |
|
Toddlers |
1.8 |
1.6 |
0.001 |
|
Symptoms: |
|||
|
Speech Delay |
1 |
1 |
1 |
|
Non-Responsive |
3.24 |
1.5 |
0.001 |
|
Poor Social Outcome |
3.48 |
1.29 |
0.001 |
|
Sensory Loss |
2.81 |
1.9 |
0.001 |
|
Repetitive Behaviour |
3.43 |
1.22 |
0.001 |
|
Behavioral Issues |
1.32 |
1.02 |
0.3 |
The first signs of ASD usually appear by the end of the first year as lack of social smile, lack
of vocalization, and babbling which normal children start at 6-8 months. The absence of
meaningful words till 16 months is also an early warning sign. However, at this stage, it is
difficult to differentiate it from other disorders. Studies point out some distinctive features
that can help in differentiating ASD from other Disorders at this stage too.18
A
stable
diagnosis of ASD by health professional is usually made in toddler age. However, most of the
children present at age of 4 when they start preschool as most of the parents get concerned when
their child does not perform well or interact with peers at school.19The mean age of
presentation in this study was also found to be 3.6 years with male preponderance. Autism is
considered to effect males more than females due to genetics underlying its
causation.20
Children with Autism Spectrum Disorder usually have different developmental trajectories than
other children. They suffer from delays in a few skills, especially in language and social
skills. While some milestones are achieved early. Most of the patients in the current study had
complaints of speech delay, repetitive behaviours and poor social interaction. Upon SGS 11
scoring speech delay was the most compromised skill with 20% of cases having severe impediment
i.e. below 3 to 5 years of their age in speech and language skills. Reinhartsen et al found that
children with ASD have more severe impairment in receptive language skills than expressive
skills when compared with children with other developmental delays. He also found such children
have more delay in their non-verbal cognitive skills.21
This was in concord with our
study where
cognitive skill was the second most compromised skill. ASD children with language delay (LD)
were found to have poorer social interaction compared to those without language delay. Also,
language delay leads to intellectual delay if early intervention is not performed. Delehanty et
al performed a detailed evaluation on toddlers with ASD, ASD with GDD, GDD alone, ASD and LD and
LD alone, and controls. He found that ASD children without GDD and LD had developmental
abilities comparable to controls. However, those with LD had more intellectual disabilities and
delayed social outcomes. Children with ASD with GDD scored significantly lower than children
having alone GDD. Therefore, special attention needs to be given to children having ASD with GDD
as they have a high risk of developing long-term disabilities.
In children less than 1 year, autism is diagnosed due to delayed achievement of speech and
milestones, which include delayed babbling, vocalization, lack of social smile, and delayed
crawling and walking (8) . However, in the current study children achieved social smiles,
babbling, and vocalization in normal time walking was delayed. This was in concord with Reindal
et al. who found the mean age of walking in children with ASD to be 15 months.22
Gender differences and their association with developmental delays in children with ASD have
shown conflicting results. Few studies reported no relationship between gender and developmental
delays.23In the current study, females scored much less than males in all domains and
had
significant deficits. A study by Zen et al. also showed females to have more emotional problems,
associated with social behavior and developmental delays.24
Another major finding in this study was the presence of global developmental delay in half of
the children withASD. Worldwide, it has a prevalence of 1-5% and in ASD children it is around
32%.25In Pakistan the rate of GDD is very high reaching up to 15%. This high
incidence is
attributed to malnutrition and maternal depression.26In the current study, the
prevalence in
children with ASD was noted to be 50%. This might be due to the high prevalence of GDD in the
country.
Among factors studied that might risk the risk of developmental delay in ASD children, only
co-morbidities were found to increase the risk of developmental delay. Studies have shown that
children with ASD have 13% lower OFC than normal children. Also, low OFC at birth is associated
with low IQ levels in ASD children.27Some studies also predict association between
obesity and
delayed development in ASD children but this was not found in our study.28However, in
our
study, this was insignificant. Among co-morbid conditions, the prevalence of epilepsy in ASD
individuals is 25-30% by time of adolescence. The presence of epilepsy is also found to be
associated with increased developmental delay and increased mortality rate in ASD
individuals.29
In the current study, 4.19% of the children had epileptic seizures. This low rate might be due
to studies not involving school children and adults.
We also studied the symptoms that might alert the physician for developmental delay assessment,
however almost all symptoms that are commonly present in autism were also present in
developmental delay. Therefore, we recommend a complete evaluation of every ASD child as they
might have associated developmental delays.
Most of the children with Autism Spectrum Disorder did not achieve developmental milestones and suffered from developmental delays. If not diagnosed timely may increase the lifetime risk of long-term disabilities therefore; attention must be given in this domain. Every ASD child must be evaluated for Developmental Delay and treated accordingly as early intervention can improve the outcome and prognosis.
- Hodges H, Fealko C, Soares N. Autism spectrum disorder: definition, epidemiology, causes, and clinical evaluation. Transl Pediatr. 2020;9(Suppl 1): S55–65. .
- Trevisan DA, Abel EA, Brackett MA, McPartland JC. Considerations About How Emotional Intelligence can be Enhanced in Children With Autism Spectrum Disorder. Front Educ (Lausanne). 2021; 6:639736
- Duvall SW, Huang L, Alison S, Hill P, Myers J, Fombonne E. No Sex Differences in Cognitive Ability in Young Children with Autism Spectrum Disorder. J Autism Dev Disord. 2020 May;50(5):1770-1785.
- Almandil NB, Alkuroud DN, AbdulAzeez S, AlSulaiman A, Elaissari A, Borgio JF. Environmental and Genetic Factors in Autism Spectrum Disorders: Special Emphasis on Data from Arabian Studies. Int J Environ Res Public Health. 2019 Feb 23;16(4):658.
- World Health Organization. Autism Spectrum Disorders. 2019
- Walensky RP, Bunnell R, Kent CK, Gottardy AJ, Leahy MA, Martinroe JC, et al. Morbidity and Mortality Weekly Report Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years-Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020 Surveillance Summaries Centers for Disease Control and Prevention MMWR Editorial and Production Staff (Serials) MMWR Editorial Board. 2020.
- Furrukh J, Anjum G. Coping with autism spectrum disorder (ASD) in Pakistan: A phenomenology of mothers who have children with ASD. Cogent Psychol. 2020;7(1): 1728108
- Ivanov I, Pacheva I, Timova E, Iordanova R, Galabova F, Gaberova K, et al. The route to autism spectrum diagnosis in pediatric practice in Bulgaria. Diagnostics. 2021;11(1):106
- Cecilia M, Vásquez M, Hernández-chávez M. Autism spectrum disorder : Clinical diagnosis and ADOS Test Trastorno del espectro autista : Diagnóstico clínico y test ADOS. 2019;90(5):485–91.
- Janvier D, Choi YB, Klein C, Lord C, Kim SH. Brief Report: Examining Test-Retest Reliability of the Autism Diagnostic Observation Schedule (ADOS-2) Calibrated Severity Scores (CSS). J Autism Dev Disord. 2022;52(3):1388-1394. .
- Mitchell C, Rt R, Rahko PS, Blauwet LA, Canaday B, Finstuen JA, et al. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults : Recommendations from the American Society of Echocardiography. Journal of the American Society of Echocardiography. 2018;32(1):1-64.
- Mohd Nordin A, Ismail J, Kamal Nor N. Motor Development in Children With Autism Spectrum Disorder. Front Pediatr. 2021; 15(9):598276.
- Wolff N, Stroth S, Kamp-Becker I, Roepke S, Roessner V. Autism Spectrum Disorder and IQ – A Complex Interplay. Front Psychiatry. 2022; 18(13):856084.
- Brown KA, Parikh S, Patel DR. Understanding basic concepts of developmental diagnosis in children. Vol. 9, Translational Pediatrics. 2020; 9(Suppl 1):S9-S22.
- Cibralic S, Hawker P, Khan F, Lucien A, Mendoza Diaz A, Woolfenden S, et al. Developmental screening tools for identification of children with developmental difficulties in high-income countries: a systematic review. Frontiers in Child and Adolescent Psychiatry. 2023;2:1074004.
- Mithyantha R, Kneen R, McCann E, Gladstone M. Current evidence-based recommendations on investigating children with global developmental delay. Arch Dis Child. 2017;102(11):1071–6.
- Silveira-Zaldivar T, Özerk G, Özerk K. Developing social skills and social competence in children with autism. International Electronic Journal of Elementary Education. 2020;13(3):341–63.
- De Giacomo A, Craig F, Palermo G, Coppola A, Margari M, Campanozzi S, et al. Differential diagnosis in children with autistic symptoms and subthreshold ADOS total score: An observational study. Neuropsychiatr Dis Treat. 2021;17:2163-2172.
- Delehanty AD, Stronach S, Slate E, Wetherby AM. Verbal and nonverbal outcomes of toddlers with and without autism spectrum disorder , language delay , and global developmental delay. 2018; 3.
- Benjamin Zablotsky, Lindsey I. Black SJB. Summary of Changes Made to the Bright Futures/AAP Recommendations for Preventive Pediatric Health Care (Periodicity Schedule). NCHS data brief. 2017.
- Reinhartsen DB, Tapia AL, Watson L, Crais E, Bradley C, Fairchild J, et al. Expressive Dominant Versus Receptive Dominant Language Patterns in Young Children: Findings from the Study to Explore Early Development. J Autism Dev Disord. 2019; 49:2447–2460.
- Reindal L, Nærland T, Weidle B, Lydersen S, Andreassen OA, Sund AM. Age of First Walking and Associations with Symptom Severity in Children with Suspected or Diagnosed Autism Spectrum Disorder. J Autism Dev Disord. 2020;50(9):3216-3232.
- Sturrock A, Marsden A, Adams C, Freed J. Observational and Reported Measures of Language and Pragmatics in Young People with Autism: A Comparison of Respondent Data and Gender Profiles. J Autism Dev Disord. 2020; 50(8):1-19.
- Zen Y, Chiyonobu T, Yuge M, Yokota I, Morimoto M, Teramukai S, et al. Gender differences in occurrence of behavioral and emotional problems at the lower grades of elementary school: Association with developmental and behavioral characteristics at 5 years. Brain Dev. 2019;41(9).
- Christensen DL, Baio J, Van Naarden Braun K, Bilder D, Charles J, Constantino JN, et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years--Autism and Developmental Disabilities Monitoring Network, 11 Sites. MMWR Surveill Summ. 2016 Apr;65(3):1–23.
- Khan MA, Owais SS, Blacklock C, Anil S, Ishaq S, Maqbool S, et al. Delivering integrated child development care in Pakistan: protocol for a clustered randomised trial. BJGP Open. 2017 Jan;1(1):bjgpopen17X100677.
- Blanken LME, Dass A, Alvares G, van der Ende J, Schoemaker NK, El Marroun H, et al. A prospective study of fetal head growth, autistic traits and autism spectrum disorder. Autism Research. 2018 Apr 1;11(4):602–12.
- Cheng W, Sun Z, Cai K, Wu J, Dong X, Liu Z, et al. Relationship between Overweight/Obesity and Social Communication in Autism Spectrum Disorder Children: Mediating Effect of Gray Matter Volume. Brain Sci. 2023 Feb 1;13(2):180.
- Tye C, Runicles AK, Whitehouse AJO, Alvares GA. Characterizing the Interplay Between Autism Spectrum Disorder and Comorbid Medical Conditions: An Integrative Review. Front Psychiatry. 2019;23(9):751
![]()
An Official
Publication of
Islamabad Medical & Dental College
Volume 12 Issue 3
Editorial
Address of Correspondence
Ramish Riaz
Email:
ramish.riaz@riphah.edu.pk
Cite this article..Waris R, Raza H, Riaz R. Patterns of Developmental Delay in Children with Autism Spectrum Disorder: A Perspective from a Developing Country. J Islamabad Med Dental Coll. 2023; 12(3): 171-178. DOI: https://doi.org/10.35787/jimdc.v12i3.814