Attitude of Physical Therapy Students Towards their Profession and Education in Punjab
Tahir Mahmood 1 , AbdulSalam 2 , Iqra Waseem 3 , Aqsa Khalid 4 , Umer Maqsood 5
1Senior Lecturer, Physical Therapist, Imran Idrees Institute of Rehabilitation Sciences, Sialkot, Pakistan.
2Assistant Professor and Head of Department, Imran Idrees Institute of Rehabilitation Sciences, Sialkot, Pakistan.
3Assistant Professor, University Institute of Physical Therapy, Lahore, Pakistan.
4Medical Officer, Sundas Foundation, Sialkot, Pakistan.
5Assistant Professor, Department of Physical Therapy, Azra Naheed Medical College, Lahore, Pakistan.
Background:The quality of medical teaching can be refined based on the attitude of the students towards their
clinical and teaching environment. The objective was to determine student attitudes towards their profession and
education in Punjab.
Methodology:TThis cross-sectional survey was conducted from 20 th July to December 2021 after taking ethical
approval. The data was collected through an online google document from physical therapy undergraduates and post
graduates from different institutes of Punjab. The outcome was measured using “physical therapy student attitudes
questionnaire (PSAQ)”.It had four sections, section A is about the knowledge of the profession, section B includes
beliefs about future, section C is about patient exposure in clinical trainings and section D is about level of satisfaction
from the learnings. The data was encoded and analyzed using SPPS V.23. The descriptive statistics and mean+
standard deviations were used to present the scores. The independent sample t-test was used to find the difference in
mean scores of males and females with p value ≤ 0.05 taken as significant.
Results: Mean age of the participants was 46.24 ± 14.13 years. Female to male ratio was 2.73:1. Almost 38.4%
patients had chronic cholecystitis, 35.2% had symptomatic gallstone disease, 24.8% had acute cholecystitis and 1.6%
had gallbladder polyps. No major vascular or common bile duct injury were observed. 27.2% patients had per
operative gallbladder perforation. Stone spillage occurred in 8.8% patients with retrieval in all of them. 75.2% patients
were discharged on day 1. Per operatively, 98.4% patients were found to have cholelithiasis, 59.6% had adhesions,
9.6% had mucocele, 1.6% had empyema and 0.8% patients had collections.
Conclusion:The student attitude was quite satisfactory regarding their choice of physical therapy profession, good
future, patient exposure and learning skills. There was no statistically significant difference based on the gender.
Keywords:Education, Patients, Physical therapy, Satisfaction, Training.
Physical therapy is a health care profession and a
part of the health care in multi-disciplinary
rehabilitation. It has an integral role in health care
system for decades. (1) This profession was started as
a three years diploma in 1963. However, there was
a demand for higher education and improved
healthcare services. (2) To meet this need,
universities started offering bachelor's degree
programs in physical therapy (PT) in the late
nineteenth century. (3) Good quality education is
necessary and reflected in the quality of physical
therapy services. To have a good physical therapy
program, it is necessary to have diverse courses,
qualified teaching staff, and well-organized clinical
training. It is shown that almost 71% of
undergraduate PT students feel that the difficulty
level of course is greater than expected. The
current educational system focuses on an
important concept called student’s satisfaction. (4) As
an academician, we can enhance students'
understanding and learning by estimation of their
satisfaction levels during their education and
learning along with clinical trainings, tools for
effective communication and proper time
management. (5) This will enable us to modify the
physical therapy program curriculum, clinical
trainings and adopt new learning strategies in our
institutions. (6) Interest in student satisfaction at
undergraduate and graduate level is well-
established within higher education in many
countries but depends upon several factors. (7) The
students’ attitude and knowledge about their
profession, results in good reputation and a
positive impact leading to social awareness and it is
other way with decreased satisfaction. (8) In this era
of emerging professions and advancement, physical
therapy profession has gained importance. There is
a need of educational foundations that enable
students to build up their skills based knowledge
and attitudes. (9, 10)
Not much studies done in Pakistan have addressed
students’ attitudes in knowledge about the
profession, beliefs about future, patient exposure
in clinical trainings and level of satisfaction from the
learnings. The objective was to estimate students’
attitudes towards their profession and education in
Punjab and find any gender-based difference. This
will help to implement new strategies for further
improvement in the profession of physical therapy.
This cross-sectional survey was conducted from 20 th
July, 2021 to 15 th December 2021 after taking
ethical approval (Ref# IIRS/DPT/IERC-372). The data
was collected online using Google document. We
included physical therapy undergraduates and post
graduates from different private institutes of
Punjab including Agile Institute Rehabilitation
sciences Bahawalpur, Bakhtawar Amin College of
Rehabilitation Sciences, Multan, Imran Idrees
Institute of Rehabilitation Sciences, Sialkot, Azra
Naheed Medical College, Lahore and University
Institute of Physical Therapy, Lahore. The
calculated sample size was 255 by applying
parameters, where, = 1.96 (Standard normal
variants at 5% type I error (p<0.05), P= 0.79
(Expected proportion in population) and d= 0.05
(absolute error). (11) The online Google document
was prepared based on the mentioned outcome
tool with addition of basic details and informed
consent, ensuring the privacy and confidentiality of
the provided responses. The outcome tool was
“physical therapy student attitudes questionnaire
(PSAQ).”It had four sections including A, 6
Questions related to the knowledge about the
profession, 5 Questions in B related to beliefs
|
Table: I Demographics of the participants (N=255) |
||
|
Descriptive Statistics |
Frequency (%ages) |
|
|
Gender |
Male |
82(32.15%) |
|
Female |
173(67.84%) |
|
|
Socioeconomic Status |
Upper Class |
19(7.45%) |
|
Middle Class |
226(88.62%) |
|
|
Lower Class |
10(3.92%) |
|
|
Professional year |
1st year |
45(17.64%) |
|
2nd year |
88(34.50%) |
|
|
3rd year |
56(21.96%) |
|
|
4th year |
38(14.90%) |
|
|
5th year |
23(9.01%) |
|
|
Masters/MPhil |
5(1.96%) |
|
|
Age Groups |
19-21 |
181(70.97%) |
|
22-24 |
68(26.66%) |
|
|
25-27 |
03(1.17%) |
|
|
28-30 |
03(1.17%) |
|
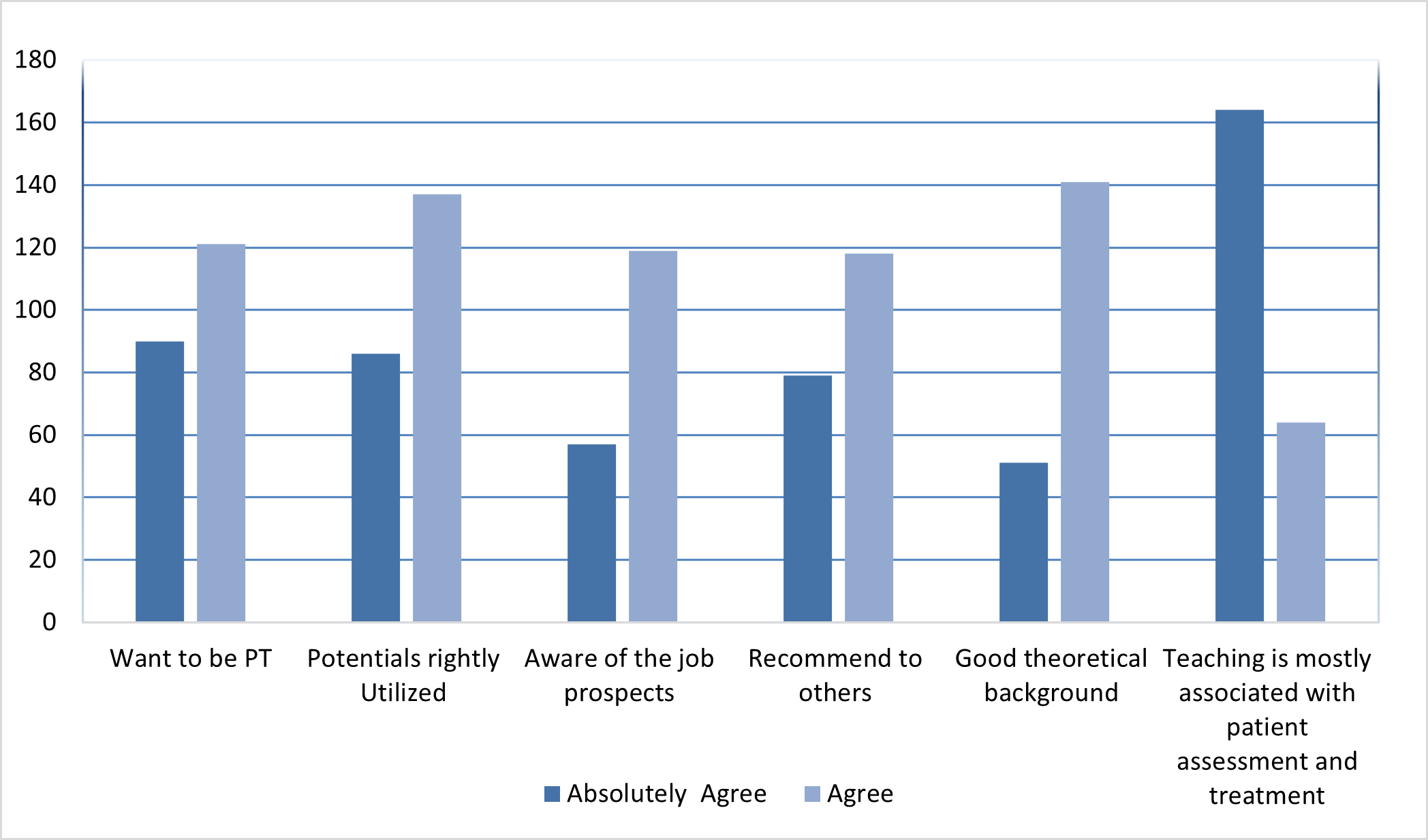
The mean age of the participants was 22.5+6.5years. The current study comprised of more females as compared to males, participants belonging to middle class were 226 (88.62%). 71.36% of the participants were from 2 nd to 4 th professional year . (Table 1) The sum of all domains of PSAQ were calculated separately. The combined scoring showed no significant gender-based difference with P value >0.05. (Table *This scoring is sum of all boxes within male and females The response of the students showed that 120 (47.05%) agree that they were willing to be physical therapist in future and 140 (54.90%) had good theoretical background, others are presented.
|
Table :II Sum of Scores and their Means |
|||||
|
Group Statistics |
|||||
|
Domain |
Gender |
N |
Mean + SD |
Std. Error Mean |
P –Value |
|
Knowledge about the profession |
Male |
82 |
21.82 + 3.84 |
.42 |
0.604 |
|
Female |
173 |
21.54 +4.10 |
.31 |
||
|
Future Beliefs |
Male |
82 |
16.63+5.44 |
.60 |
0.244 |
|
Female |
173 |
17.45+5.11 |
.39 |
||
|
Patient exposure in clinical trainings |
Male |
82 |
24.55+5.60 |
.62 |
0.873 |
|
Female |
173 |
24.43+5.68 |
.43 |
||
|
A- Level of satisfaction from the learnings. |
Male |
82 |
24.62+5.56 |
.61 |
0.944 |
|
Female |
173 |
24.57+6.08 |
.46 |
||
|
All |
Male |
82 |
87.62+17.64 |
1.95 |
0.844 |
|
Female |
173 |
87.98+18.67 |
1.42 |
||
Laparoscopic cholecystectomy is the treatment of
choice and gold standard due to less pain,
minimum surgical trauma, short postoperative
hospital stay and early return to home. In our
study, female to male ratio was 2.7:1 (73.2% vs
26.8%) which shows less female predominance as
compared to another study conducted in Pakistan. 15
This may represent a changing trend of
cholelithiasis, becoming more common in males in
our region owing to dietary changes over recent
times. However, the female predominance itself is
consistent with international data. 16 Mean age in
our study was 46 years which is consistent with
regional and international studies. 15,16 In terms of
presentation or indication for surgery, 38.4%
patients had chronic cholecystitis, 35.2 % had
symptomatic gallstone disease, 24.8% had acute
cholecystitis and 1.6% had gallbladder polyps. This
is consistent with the study done in Pakistan. 15
Mostly bleeding in laparoscopic cholecystectomy
occurs from trocar site insertion, liver bed
(especially in cases of acute cholecystitis and
empyema gallbladder) and vascular injury (usually
cystic duct or its branches or anomalous vessel). In
rare cases, massive bleed can occur due to injury to
abdominal aorta, vena cava, iliac vessels, hepatic
artery or portal vein. 17 In our study, 72% patients
had less than 50ml blood loss, 22% patients had 51
to 150 ml blood loss and 6% patients had more
than 150ml blood loss. There was no major vascular
injury in our study. 27.2% patients had per
operative gallbladder perforation resulting in bile
spillage. It is less as compared to an international
study that reported gallbladder perforation in
36.1% patients. 18 It is variably common in 10 to 30%
of laparoscopic cholecystectomies, but it is usually
not associated with any dreadful outcome, surgical
site infection or post-operative collection. 19 Suction
irrigation of the contaminated area is sufficient to
address it. Stone spillage occurred in 8.8% patients
in our study. Spilled stones can be culprits for
abdominal collection, abscess formation, pain ileus
etc. To avoid these, stone retrieval was performed
in all of such cases followed by lavage. Additionally,
clips were applied from where the spillage started,
to prevent further contamination and spillage.
Acutely inflamed and over distended gall bladders
were main factors for this intraoperative event. No
common bile duct injury was noted. This is
consistent with studies done in Karachi and
Peshawar. 20,21 The incidence of common bile duct
injury is strongly related to exposure of Calot’s
triangle, experience, knowledge and proper training
of a laparoscopic surgeon. It is one of the most
dreadful complications while performing
laparoscopic cholecystectomy. 15 High morbidity,
mortality, and prolonged hospitalization is
associated with common bile duct injury. 22
Accessory cystic duct was noted in two cases. This
is a unique finding and requires active per operative
vigilance to recognize it which otherwise will
present as bile leakage and related complications.
There are few cases of accessory cystic duct
reported internationally. 23,24 75.2% patients were
discharged on day 1 which is a routine worldwide in
good laparoscopic centers. Patients requiring two
or more days were mostly cases of acute
cholecystitis, biliary pancreatitis or those who
needed time for decision or second opinions with
family and doctors regarding surgery in acute
cholecystitis, empyema gallbladder etc.
Comorbidities included hypertension 19.2%,
diabetes mellitus 12%, hepatitis C 3.6%, ischemic
heart disease 2.4%, tuberculosis 1.2%,
asthma/chronic obstructive lung disease 0.8% and
hepatitis B 0.4%They were optimized with proper
specialist consultations accordingly prior to surgery.
This was a single-center study and retrospective in
nature as all the data was collected from the past
records that limits its quality. Multi-centered study
with a larger sample size would have increased
generalizability. Same surgeon performing all the
operations adds to benefit on one side but also
adds the bias to the study. It is pertinent to see the
outcomes when another specialist performs the
surgery with the same team. This study has
provided evidence for improving surgical practices
and demonstrated that proper training and
experience decreases the risk of intraoperative
complications and high end laparoscopic setup and
vigilance improves the outcomes.
Laparoscopic cholecystectomy is a safe procedure in all types of gallstone disease presentations with a low complication rate.
- Ahmad G, Baker J, Finnerty J, Phillips K,Watson A. Laparoscopic entry techniques. The Cochrane Library. 2019;1(1):CD006583. doi: 10.1002/14651858.CD006583.pub5
- Jaschinski T, Mosch C G, Eikermann M, Neugebauer E.A, Sauerland S. Laparoscopic versus open surgery for suspected appendicitis. Cochrane Database of Systematic Reviews. 2018;11(11):CD001546. doi: 10.1002/14651858.CD001546.pub4
- Balogun O S, Osinowo A O, Olajide T O, Lawal A O, Adesanya A, Atoyebi O A, et al. Development and practice of laparoscopic surgery in a Nigerian tertiary hospital. Nigerian Journal of Clinical Practice. 2020;23(10):1368–1374. doi: 10.4103/njcp.njcp_125_20
- Târcoveanu E, Vasilescu A, Lupaşcu C, Vlad N, Moraru M, Stanciu C,et al. Laparoscopic cholecystectomy in cirrhotic patients. Chirurgia (Bucharest, Romania: 1990). 2020;115(2):213-219. doi: 10.21614/chirurgia.115.2.213
- Loozen C. S, van Santvoort H. C, van Duijvendijk P, Besselink M. G, Gouma D. J, Nieuwenhuijzen G. A, et al.Laparoscopic cholecystectomy versus percutaneous catheter drainage for acute cholecystitis in high risk patients (CHOCOLATE): multicentre randomised clinical trial. BMJ (Clinical Research Ed.). 2018;363:k3965 doi: https://doi.org/10.1136/bmj.k3965
- Xu Y, Wang H,Yang, M. Preoperative nursing visit reduces preoperative anxiety and postoperative complications in patients with laparoscopic cholecystectomy: A randomized clinical trial protocol: A randomized clinical trial protocol. Medicine. 2020;99(38):e22314. doi:10.1097/MD.0000000000022314
- Amreek F, Hussain S. Z. M, Mnagi M. H, Rizwan, A. Retrospective analysis of complications associated with laparoscopic cholecystectomy for symptomatic gallstones. Cureus. 2019;11(7):e5152. doi: 10.7759/cureus.5152
- Donmez, T, Erdem, V. M, Uzman S, Yildirim D, Avaroglu H, Ferahman S, et al.Laparoscopic cholecystectomy under spinal-epidural anesthesia vs. general anaesthesia: a prospective randomised study. Annals of Surgical Treatment and Research. 2017;92(3):136–142. doi.org/10.4174/astr.2017.92.3.136
- Panagiotopoulou IG, Carter N, Lewis MC, Rao S. Early laparoscopic cholecystectomy in a district general hospital: is it safe and feasible? Int J Evid Based Health. 2012;10(2):112–6. doi: 10.9738/INTSURG-D- 13-00068.1 Hayama S, Ohtaka K, Shoji Y, Ichimura T, Fujita, M, Senmaru N, et al. Risk factors for difficult laparoscopic cholecystectomy in acute cholecystitis. Journal of the Society of Laparoendoscopic Surgeons. 2016;20(4):e2016.00065. doi: 10.4293/JSLS.2016.00065
- Dalwani AG, Shaikh R, Das K, Devrajani T, Shah SZA, Shah A. Complications of Laparoscopic Cholecystectomy at Liaquat University, Jamshoro. World Appl Sci J. 2013;23(6):808–11. doi: 10.5829/idosi.wasj.2013.23.06.747
- Isazadehfar K, Entezariasl M, Shahbazzadegan B, Nourani Z, Shafee Y. The Comparative Study of Ondansetron and Metoclopramide Effects in Reducing Nausea and Vomiting After Laparoscopic Cholecystectomy. Acta Medica Iranica. 2017;55(4):254-258. PMID: 28532137 Protic M, Veljkovic R, Bilchik AJ, Popovic A, Kresoja M, Nissan A, et al. Prospective randomized controlled trial comparing standard analgesia with combined intra-operative cystic plate and port-site local anesthesia for post-operative pain management in elective laparoscopic cholecystectomy. Surg Endosc. 2017;31(2):704-713. doi: 10.1007/s00464-016-5024- 5.
- Farooq Umar, Rashid Tariq, Naheed Asma, Barkat Najeeb, Iqbal Muhammad, Sultana Qamar. Complications of laparoscopic cholecystectomy. J Ayub Med Coll Abbottabad 2015;27(2):407-410. PMID: 26411129
- Afzal M, Rehman S, Butt M. Q. Complications of laparoscopic cholecystectomy: An analysis of 400 consecutive cases. Pak Armed Forces Med J.2014;64(4):546-50. www.pafmj.org/index.php/PAFMJ/article/view/1399 Shah MY, Somasundaram U, Wilkinson T, Wasnik N. Feasibility and Safety of Three-Port Laparoscopic Cholecystectomy Compared to Four-Port Laparoscopic Cholecystectomy. Cureus. 2021;13(11):e19979. doi: 10.7759/cureus.19979
- Desai GS, Pande P, Narkhede R, Kulkarni DR. Revision Roux-en-y hepaticojejunostomy for a post- cholecystectomy complex vasculobiliary injury with complete proper hepatic artery occlusion: A case report and literature review. Int J Surg Case Rep. 2019;58:6-10. doi: 10.1016/j.ijscr.2019.03.032 Altuntas YE, Oncel M, Haksal M, Kement M, Gundogdu E, Aksakal N, et al. Gallbladder perforation during elective laparoscopic cholecystectomy: Incidence, risk factors, and outcomes. North Clin Istanb. 2018;5(1):47-53. doi: 10.14744/nci.2017.88155
- Evans L, Sams E, Naguib A, Hajibandeh S, Hajibandeh S. Iatrogenic gallbladder perforation during laparoscopic cholecystectomy and outcomes: a systematic review and meta-analysis. Langenbeck's Archives of Surgery. 2022;407(3):937-946. Doi: 10.1007/s00423-022-02439-2 Kerawala AA, Bakhtiar N, Qureshi NA. Laparoscopic cholecystectomy by resident is safe. RMJ. 2019;44(03):634-636.
- Shah RU, Shah S, Qazi M, Shiraz DA, Ullah HN, Kalim M. Outcome of laparoscopic cholecystectomy in terms of complications in Lady Reading Hospital Peshawar. Professional Med J. 2022;29(06):859-863. doi: 10.29309/TPMJ/2022.29.06.6639
- Halbert C, Altieri MS, Yang J, Meng Z, Chen H, Talamini M, et al. Long-term outcomes of patients with common bile duct injury following laparoscopic cholecystectomy. Surg Endosc. 2016;30:4294-4299. doi: 10.1007/s00464-016-4745-9 Wu CH, Wu PW, Wong YC, Kang SC. Diagnosis of a single gallbladder with double cystic ducts and dominant accessory duct draining into the right hepatic duct: a case report. J Int Med Res. 2021;49(11):3000605211053981. doi:10.1177/03000605211053981
- Munie S, Nasser H, Go PH, Rosso K, Woodward A. Case report of a duplicated cystic duct: A unique challenge for the laparoscopic surgeon. Int J Surg Case Rep. 2019;56:78-81. doi:10.1016/j.ijscr.2019.02.030
![]()
An Official Publication of
Islamabad Medical & Dental College
Volume 11 Issue 3
Editorial
Address of Correspondence
Tahir Mahmood
Email:
tahirmahmoodphysio@gmail.com
Mahmood T, Salam A, Waseem I, Khalid A, Maqsood U. Attitude of Physical Therapy Students Towards their Profession and Education in Punjab. J Islamabad Med Dental Coll. 2022;11(3): 182-187 DOI: https://doi.org/10.35787/jimdc.v11i3.851