A Descriptive Correlational Study of Vascular Foramina in Adult Human Femora in Cadavers in Pakistan
Arsalan Manzoor Mughal1Tehzeeb Ul Hassan2Beenish Sabir3Hafsa Arshad Azam Raja4Sheikh Mohammad Ahmad5
1Assistant Professor, Department of Anatomy, Rawalpindi Medical University, Pakistan
2Head of Department, Anatomy, Rawalpindi Medical University, Pakistan
3,4,5 2nd Year MBBS, Rawalpindi Medical University, Pakistan
Objective: This study was conducted to study the variations in the number and location of nutrient and epiphyseal vascular foramina of the femur in the Pakistani population
Methodology:This descriptive cross-sectional study was conducted from April -June '2022 after getting ethical approval. Data collection tool: 24-gauge hypodermic needles & measuring tapes.
Data collection and Analysis: SPSS & Excel
Inclusion & exclusion criteria: Anatomically sound bones were included from the bone bank of RMU; pathological, deformed bones were excluded
Results:Out of 80 bones 66.6% had single nutrient foramina, whereas 31.3% had two on the shaft. 82.05% of foramina were type II, 16.67% were type I and 1.26% were type III. Only 2.5% had no foramina. Majorly the nutrient foramina were found on the medial surface, medial lips or between the lips of linea aspera. There was no significant difference bilaterally in the mean foraminal index, foraminal length, or several epiphyseal vascular foramina, which were 18.65 cm, 42.66 cm, and 16 cm respectively.
Conclusion: Most of the nutrient foramina in the femora were found in the middle third of the shaft, either on the medial lip of the Linea Aspera or on the shaft’s medial surface; however, variations in their location have been found. The mean epiphyseal vascular foramen ranged from 6 to 26.
The article finds its implications in orthopaedic surgery and osteogenesis.
Key words:Epiphyses, Diaphysis, Femur, long bones, Hip joint, Arteries, Pathology, Research, osteogenesis, Population
In humans, the femur is a long bone that articulates with the acetabulum to form the hip joint. Blood supply to the femur is via epiphysial arteries & nutrient arteries. The femur is well supplied by many arterial groups named diaphyseal, epiphyseal, metaphyseal, and periosteal arteries.1 The main blood supply for the femoral shaft is the nutrient artery, a branch of the second perforating branch of the profunda femoris artery or from the 1st perforating branch. Sometimes, additional nutrient arteries may supply the femur from either of the rest of the perforating arteries.2 It permits the nutrient artery to enter obliquely piercing the bone’s periosteum and entering the osteon via the haversian system reaching the medullary cavity. The diaphyseal artery’s entry and angulation is specific representing the direction of the growing end in most long bone.4 Nutrient foramen are usually located on the shaft and may be up to three for a single bone usually near the Linea Aspera in the upper 2/3rd region.5,6 Aging and certain pathological conditions such as anaemias, diabetes, chronic airway diseases, tumours, as well as immobility result in a decline in the quality of blood supply to all bones including the femur. The position of the nutrient foramen is significant for morphological, pathological, and operative procedures such as microvascular bone grafts.8
Additionally, the femur’s upper end is rich in blood supply due to the many branches of several main arteries that anastomose with each other. The head of the femur gets its blood supply mainly via retinacular arteries from the medial circumflex branch of the profunda femoris artery.9 The other source to the head are the vessels from the obturator artery and the pericapsular anastomoses that provide blood supply to the hip joint too.10 Retinacular arteries that are derived from trochanteric anastomosis around the greater trochanter supply the intra-capsular part of the femoral neck. The cruciate anastomosis is another source which is formed by the ascending branch of 1st perforating artery, the inferior gluteal artery’s descending branch, and the circumflex femoral arteries. The rich vascular supply through the retinacula of Weitbrecht via a large number of retinacular vascular foramina in the neck region can be explained based on the fact that these vessels ensure the optimal vascularity of the hip joint.2
Although much research has been done on the diaphyseal nutrient foramina of the femur, scant literature is available on the locations and number of epiphyseal vascular foramina a few of which are from our region. So, this research was designed to study the variations in nutrient and epiphysial vascular foramina of the femur in the Pakistani population.
For this descriptive cross-sectional study, Pakistani femora of unspecified gender and age were acquired. Data was collected from April 2022 to June 2022. Only anatomically sound bones were used in the study. Bone having anatomical or physical pathology and deformity were not used in the study.
24-gauge hypodermic needles and magnifying hand lenses were used for determining the Diaphyseal nutrient foramina and epiphyseal vascular foramen. All the bones were examined macroscopically in a well-illuminated area. The nutrient foramen was identified as it has a distinct groove along with a little-raised area at the beginning of the canal.11 This was verified by passing a 24-gauge needle from the cortex into the medullary. (fig. 1a) For the bone having two foramina, the bigger and more prominent one was considered the primary or dominant and the smaller one was considered the secondary foramen. passed through the canal. Epiphyseal vascular foramina were counted using a handheld magnifying lens. (fig. 1d).
It was calculated by Hughes's Formula. For femora having two nutrient foramen, the larger one was considered to calculate the foraminal index.12
The distance of the nutrient foramen was calculated by marking the upper margin of the head and measuring the distance to the location of the nutrient foramina. If a femur had two nutrient foramina, the larger one was considered for the calculation. The distance between these two points was marked using markers and measured with a measuring tape. (fig. 1b)
The total bone length was calculated by marking two points on the plane paper that indicated the outermost margin of the bone. The upper margin was drawn at the superior-most limit of the head, while the lower margin was drawn from the inferior-most level of the medial condyle of the bone. The distance between these two points indicated the total femur length, which was then measured in centimetres using the meter rule. (fig. 1c)
According to the foraminal index, the nutrient foramina were divided into three main categories; Type 1 with a foraminal index of less than 33.3%, type 2 with a foraminal index between 33.33% - 66.66% and type 3 with a foraminal index above 66.66%.
Frequency and percentages were calculated for qualitative variables such as the location of Diaphyseal Nutrient foramen and foraminal position type. Means and standard deviations were calculated for quantitative variables such as the distance of Nutrient foramen from the proximal end, the number of Epiphyseal Vascular Foramen, and the Foraminal Index. Student’s t-test was used to compare the difference in means between the left and right femora for these variables. Pearson’s correlation was used to determine the association between the number of vascular foramina and shaft length.
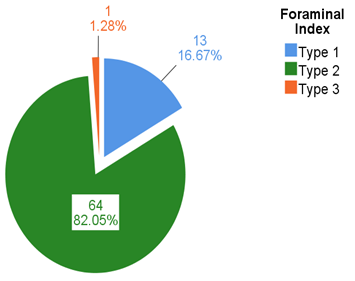
Eighty anatomically intact adult femora were taken from the Rawalpindi Medical University’s bone bank and the location of nutrient foramina was studied. Thirty-five bones were on the right side and forty-five bones were on the left side. Fifty-three bones (66.6%) had single nutrient foramina whereas twenty-five bones (31.3%) had two nutrient foramina on the shaft. Most (82.05%) of foramina were type II, 16.67% were type I and 1.26% were type III. (Fig 2) Only two bones (2.5%) had no nutrient foramina.
|
Table I: Location of nutrient foramen of femur |
||
|
Location of nutrient foramen |
Frequency |
Percentage |
|
Linea Aspera |
12 |
11.7 |
|
Linea Aspera’s medial lip |
29 |
28.6 |
|
Medial surface |
26 |
25.2 |
|
Between Medial and Lateral Lips of Linea Aspera |
20 |
19.1 |
|
Linea Aspera’s lateral lip |
10 |
9.7 |
|
On Lateral Surface |
6 |
5.8 |
|
Total |
103 |
100.0 |
|
Table II: The number of Epiphyseal Vascular Foramen, Distance of Nutrient foramen from the proximal end, and Foraminal Index . |
||||||||
|
Vascular Foramen Parameters |
Side |
N |
Mean |
Std. Deviation |
P-Value |
|||
|
Nutrient Foramen distance from Proximal End (cm) |
Right |
35 |
18.39 |
5.46 |
0.709 |
|||
|
Left |
45 |
18.85 |
5.49 |
|||||
|
Total |
80 |
18.65 |
5.45 |
|||||
|
Foraminal Index |
Right |
35 |
42.69 |
12.50 |
0.983 |
|||
|
Left |
45 |
42.63 |
12.06 |
|||||
|
Total |
80 |
42.66 |
12.18 |
|||||
|
Epiphyseal Vascular Foramen (Neck) |
Right |
35 |
16 |
10 |
0.964 |
|||
|
Left |
45 |
16 |
11 |
|||||
|
Total |
80 |
16 |
10 |
|||||
|
|
||||||||
|
Table III: Correlation between the number of vascular foramina and shaft length |
||||||||
|
Variable |
Nutrient Foramina on Diaphysis |
Epiphysial Vascular Foramen on Neck |
||||||
|
Shaft Length(cm) |
Pearson Correlation |
-.034 |
.082 |
|||||
|
P Value |
.770 |
.468 |
||||||
|
N |
78 |
80 |
||||||
From the proximal end, the mean distance of the nutrient foramen was 18.65±5.45 cm difference between the sides being insignificant. The mean foraminal index was 42.66±12.18 with the difference between the sides being insignificant. The mean number of epiphyseal vascular foramen was 16±10 which was also not significant between the right and left sides. (Table 2) The correlation between shaft length and the number of vascular foramina in the shaft or the epiphysis was also not significant. (Table 3)
Despite the immense popularity of open reduction surgery in femoral shaft fracture, there’s little research on all the required details of the femoral blood supply. An adequate knowledge of the nutrient vessels' anatomy and their entry into the bone is of great significance as the success of these operations depends significantly upon the preservation of the bone’s blood supply.
According to Hughes, Femur is a long bone with the most varied nutrient foramen. 13 These range from absent nutrient foramina to a maximum of three. Most researchers have reported that femora often contain single nutrient foramen.14 In our study a single nutrient foramen was found in 66.6% of the femora. Mysorekar, Prashanth and others have reported two nutrient foramina in 42 to 55% of femora contain double nutrient foramina, 15,16 However, our research on Pakistani femora revealed that 31.3% of bones had two nutrient foramina, indicating that two main diaphyseal nutrient arteries are supplying the shaft in these bones. Few studies have reported up to three nutrient foramen with an only 3.5% of incidence; however, none of the bones we studied had three nutrient foramina.12 Maximum number of reported foramina is nine but this is extremely rare. 17
We found only two bones (2.5%) that had no nutrient foramina. In another research, 4.6% of 86 femora had absent foramina.16 The absence of nutrient foramen is not enigmatic; it’s indicative of the fact that a nutrient artery might not have developed during intrauterine life. There might have been defects in vasculogenesis and angiogenesis during embryonic life that prevented the development of diaphyseal nutrient arteries in 2.5% of the femora. When a bone lacks the main nutrient artery, it’s usually supplied by the periosteal arteries.12 However, due to rich anastomosis between periosteal, epiphyseal, and other small diaphyseal arteries, adequate nutrition to the bone is maintained through it. Although the compensation is done well by these vessels it still may not supply the bone optimally. It results in impaired osteogenesis and avascular necrosis during the fractures of the femur.1 To minimize the chances of delayed or non-union fracture, an orthopaedic surgeon must have adequate knowledge regarding the morphology of nutrient foramen.18
The geographical area also has a subjective influence on the nutrient foramina location. We found nutrient foramen mostly on the medial surface, medial lips of linea aspera or between the lips of linea aspera. None were found on the lateral surface with the difference between the sides being insignificant. Similarly, in North Indians, the nutrient foramen is found in abundance in the interstice, followed by on the Linea Aspera’s medial lip, which is in congruence with our study. 19 In the Black South African population reported a similar pattern but in the white South Africans, most nutrient foramina are placated on the Linea Aspera and sometimes on the posterolateral surface.20 In the Turkish population, the right femora have a higher frequency of nutrient foramen on the medial lip whereas it changes to the lateral lip in the left femora.21 In the Nepalians, the nutrient foramina are found abundantly on the lateral surface. 22
This precise knowledge about epiphyseal retinacula foramen is important in performing surgeries around the upper end of the femur i.e., hip fracture and hip dislocation surgeries. Lateral ascending cervical branches of the Medial circumflex humeral artery can be disrupted easily and can cause avascular osteonecrosis. In a sample of 76 Chinese cadaveric bones, they counted 2417 vascular foramina most of which were on the superior aspect, anterior and posterior surfaces of the neck.7 This study complies with reports from Lavigne et al.23 These studies reported the presence of nutrient foramina in the anterolateral regions of the neck; however, Lavigne et al. also have reported that 71% of femora contain no nutrient foramina in the anterior regions. We found 1303 vascular foramina on the neck region in 80 bones -which is markedly less than the Chinese. Most of these retinacular foramina were found on the neck’s posterior side whereas some were located on the superior surface and intertrochanteric crest. It’s likely to hypothesize that these variations in Chinese could be due to greater physical activity compared to our population. Having a better nutritional status can also be a factor as Meiguei Angel Medina and Ana R. Quesada have suggested a correlation between the modulatory effects of dietary protein and angiogenesis.24 Different opinions exist regarding the relationship between the total bone length to the size or number of vascular foramina in the femoral neck. Some have reported that there is no association between the distribution of nutrient foramen with the length of the bone.12,21 However, Jiong Mei has reported that the length of the bone and the number of vascular foramina on the neck are positively correlated. 25 No correlation between the two variables was found in our study. Larger prospective studies should be done to study this phenomenon. The number of retinacular foramina has clinical significance because, in individuals with fewer vascular foramina located near the articular cartilage, even a mild fracture i.e., valgus-impacted fractures of the neck may lead to the head’s avascular necrosis. Limitations of our study were that age and gender differences were not taken into account as these bones were obtained from the bone bank. Further study can be done to study these parameters where data is available.
Nutrient foramen in the femora of the Pakistani population is commonly found on the shaft’s middle third, Lina Aspera’s medial lip, the shaft’s medial surface or between the two lips of Linea Aspera. However, some variations in their location have been found in this study. The mean epiphysial vascular foramen per bone ranged from six to twenty-six but no correlation was found with bone length.
- Arias DG, Marappa-Ganeshan R. Anatomy, bony pelvis and lower limb, arteries. Susan S. Gray’s anatomy: the anatomical basis of clinical practice. https://doi.org/10.1002/ca.22677 Karmali NK, Chouhan SK. A morphological study of position of nutrient foramen in dry human femur. International Journal Of Scientific Study. 2019;7(3):75-8.
- Paul RG, Navin Kumar Balla I, SailajaT K. Variations Of The Nutrient Foramina In Dried Human Femur. Orig Res Artic. 2019;7(1):6780–5. https://doi.org/10.16965/ijar.2019.224 Dervisevic L, Dervisevic A, Ajanovic Z, Hasanbegovic I. Analytical and morphometric study of nutrient foramina of femur and its clinical implications. International Journal of Research in Medical Sciences. 2019 Apr;7(4):1324. https://doi.org/10.18203/2320-6012.ijrms20191347
- Murali Krishna S, Kumar U, Sirisha V, Rajesh V. Morphologic and morphometric study of the nutrient foramina in dry human femur bones of Telangana region. Int J Anat Res. 2016;4(2):2464-68. https://doi.org/10.16965/ijar.2016.239 Mei J, Ni M, Wang G, Jia G, Liu S, Cui X, et al. Number and distribution of nutrient foramina within the femoral neck and their relationship to the retinacula of Weitbrecht: an anatomical study. Anat Sci Int. 2017 Jan;92(1):91–7. https://doi.org/10.1007/s12565-015-0319-5
- M Murlimanju BV, Prashanth KU, Prabhu LV, Saralaya VV, Pai MM, Rai R. Morphological and topographical anatomy of nutrient foramina in human upper limb long bones and their surgical importance. Rom J Morphol Embryol. 2011 Mar;52(3):859-62.
- Prashanth KU, Murlimanju B V., Prabhu L V., Kumar CG, Pai MM, Dhananjaya KVN. Morphological and topographical anatomy of nutrient foramina in the lower limb long bones and its clinical importance. Australas Med J. 2011;4(10):530–7. https://doi.org/10.4066/amj.2011.725
- Karmali NK, Chouhan SK. A morphological study of position of nutrient foramen in dry human femur. International Journal Of Scientific Study. 2019;7(3):75-8.
- Prashanth KU, Murlimanju B V., Prabhu L V., Kumar CG, Pai MM, Dhananjaya KVN. Morphological and topographical anatomy of nutrient foramina in the lower limb long bones and its clinical importance. Australas Med J. 2011;4(10):530. https://doi.org/10.4066/amj.2011.725
- Ukoha UU, Umeasalugo KE, Nzeako HC, Ezejindu DN, Ejimofor OC, Obazie IF. A study of nutrient foramina in long bones of Nigerians. National journal of medical research. 2013 Dec 31;3(04):304-8.
- Lazaro LE, Klinger CE, Sculco PK, Helfet DL, Lorich DG. The terminal branches of the medial femoral circumflex artery: the arterial supply of the femoral head. The bone & joint journal. 2015 Sep;97(9):1204-13. https://doi.org/10.1302/0301-620x.97b9.34704
- Mei J, Quan K, Wang H, Dai Y, Zhang F, Ni M. Total cross-sectional area of the femoral neck nutrient foramina measured to assess arterial vascular beds in the femoral head. J Orthop Surg Res. 2019 Dec;14(1):1–7. https://doi.org/10.1186/s13018-019-1480-7
![]()
An Official Publication of
Islamabad Medical & Dental College
Volume 12 Issue 4
Editorial
Address of Correspondence
Arsalan Manzoor
Email:
arsalanmanzoor@gmail.com
Cite this article.Mughal A M, Hassan T U, Sabir B, Raja H A A, Ahmad S M. A Descriptive Correlational Study of Vascular Foramina in Adult Human Femora in Cadavers in Pakistan .J Islamabad Med Dental Coll. 2022; 12(2): 140-146 DOI: https://doi.org/10.35787/jimdc.v12i2.927